Post-thoracotomy pains are the worst post-operative pains, occurring in high frequency and can be severe. Surprisingly, asthma beta-adrenergic stimulants greatly reduce any neuropathic pain, though not muscular pains, postsurgery. It suggest beta-adrenergic circuits, thought to be involved in descending inhibition, might be important.
I wrote about how beta-adrenergic agents might be involved in downward inhibition:
Antidepressants Just Don’t Work on Descending Inhibition
http://painmuse.org/?p=3241
The fact beta-adrenergic agents prevent post thoracic neuropathic pains here:
Eur J Pain. 2015 Nov;19(10):1428-36. doi: 10.1002/ejp.673.
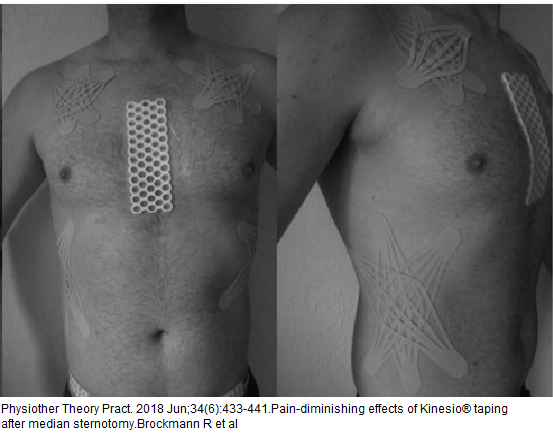
Effects of β2 agonists on post-thoracotomy pain incidence.
Salvat E et al
https://www.ncbi.nlm.nih.gov/pubmed/25766791
“The chronic use of β2 -agonists was an independent predictor of thoracic neuropathic pain (but not of non-neuropathic pain) and was associated with a five-fold decrease in the relative incidence of neuropathic pain [OR = 0.19 (0.06-0.45)].”
beta adrenergic agents were found to work as well as antidepressant in animal model of diabetic neuropathy:
Choucair-Jaafar, Nada, et al.
The antiallodynic action of nortriptyline and terbutaline is mediated by β2 adrenoceptors and δ opioid receptors in the ob/ob model of diabetic polyneuropathy.
Brain research 1546 (2014): 18-26.
https://www.sciencedirect.com/science/article/pii/S0006899313015631

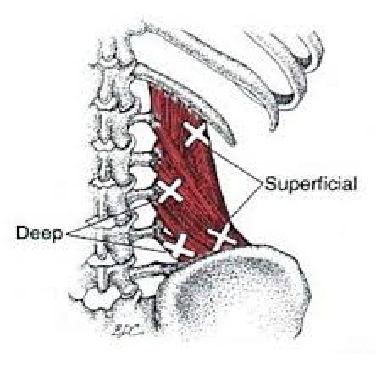 (Travell & Simon)
(Travell & Simon)