
POT’s is a syndrome where one is unable to maintain blood pressure standing and so often faint – and is often associated with attacks of tachycardia.
Finding this situation in a chronic pain patient, greatly complicates the situation, and makes pain recovery less likely. I find myself scratching my head about where to go because so many possible contributors.
SUMMARY:
- Association of POTS with autonomic neuropathy brings up issue that certain Fibromyalgia cases have small fiber neuropathy. Autoimmune mechanisms are involved and question lies, which ones would respond to IV gamma globulins or Plasmaphoresis – certainly the ones with frank Chronic Demyelinating Inflammatory Polyneuropathy (CIDP) but what about milder forms? Prednisone steroid pulses work in early CRPS and could help some autonomic neuropathy (certainly in CIDP) – but when to try? Measuring certain antibodies might help but in some situations testing is rare or unavailable.
- Association of a case of POTS with chairi malformation brings up association of certain FM cases with treatable chairi syndrome cases. Our MRI testing is either unavailable or untrustworthy.
- Large association of POTS with Ehlers-Danlos hypermobility syndrome makes pain issues much more likely. Saw one case of CRPS caused by superficial radial nerve injury from unstable distal radius. Does one dare try prolotherapy to an already painful site?
- Body- wide serotonin in POTS is low and POTS is associated with high suicide risk, adding a deeply troubling challenge to pain in POTS cases.
- Treatment of associated sleep apnea with CPAP may be complicated. Ordinary CPAP might not work and BIPAP might need to be tried. The anxiety that is associated might limit mask use and in one case, clonazepam 1 mg hs had to be used to reduce nightmares and ensure CPAP use.
- Cases are found of CRPS and POTS helped by treatment of bacterial overgrowth. Is this why Cefadroxil antibiotic cured one CRPS case?
- Using Naltreoxone dual opioid blocker /mild stimulator could help CRPS and POTS but how does one get subjects off opioids first?
- Rare POTS cases found deficient in thiamine, B12 and Vitamin D offer rare cures. These deficiencies also flare Fibromylagia. Treatment of the POTS with local measures and Flourinef and or Midodrine can help.
- New finding of having Normal blood B12 levels with non-existent Brain Fluid B12 levels in autoimmune victims adds another level of complexity to issue (writing it up soon)
__________________________________________________
I would first suggest that any chronic pain condition might effect orthostatic tolerance – for example in Chronic Pelvic pain this is found more likely:
Chelimsky, Gisela, et al.
Autonomic testing in women with chronic pelvic pain.
The Journal of urology 196.2 (2016): 429-434.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4969223/pdf/nihms797039.pdf
- 37% orthostatic intolerance.
Secondly, autonomic dysfunction can be determined through a COMPASS31 questionnaire:
Mayo Clin Proc. 2012 Dec;87(12):1196-201.
doi: 10.1016/j.mayocp.2012.10.013.
COMPASS 31: a refined and abbreviated Composite Autonomic Symptom Score.
Sletten DM(1), Suarez GA, Low PA, Mandrekar J, Singer W
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3541923/
actual form is here:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3541923/bin/mmc2.pdf
I will attack each issue mentioned in intro in turn:
Small Fiber Neuropathy – Autonomic Neuropathy
Association of POTS with autonomic neuropathy brings up issue that certain Fibromyalgia cases have small fiber neuropathy. Autoimmune mechanisms are involved and question lies, which ones would respond to IV gamma globulins or Plasmaphoresis – certainly the ones with frank Chronic Demyelinating Inflammatory Polyneuropathy (CIDP) but what about milder forms? Prednisone steroid pulses work in early CRPS and could help some autonomic neuropathy (certainly in CIDP) – but when to try? Measuring certain antibodies might help but in some situations testing is rare or unavailable.
-
“POTS is present in higher frequency in patients with other autoimmune disorders such as multiple sclerosis”
Kanjwal, Khalil, et al.
“Autonomic dysfunction presenting as postural orthostatic tachycardia syndrome in patients with multiple sclerosis.”
International journal of medical sciences 7.2 (2010): 62.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2840604/ - high incidence of Fibromyalgia(FM) in POTS:
Chemali, Kamal, and Kevin Mc Neeley.
Co-Morbidities of Neuropathic Postural Orthostatic Tachycardia Syndrome and of the Autonomic Neuropathies (P1. 093).
Neurology 82.10 Supplement (2014): P1-093.
http://n.neurology.org/content/82/10_Supplement/P1.093.short
“The high prevalence of disorders such as Fibromyalgia and CFS in both POTS and AN [autonomic neuropathy], may point to a role of the ANS[autonomic neuropathy syndrome] in these conditions.” - A subgroup of POTS and a subgroup of Hypermobility cases have small fiber neuropathy:
Iodice, V., et al.
Small fibre neuropathy and Collagen IV reduction in Postural Tachycardia Syndrome and Joint Hypermobility Syndrome.
Autonomic Neuroscience: Basic and Clinical 192 (2015): 125.
http://www.autonomicneuroscience.com/article/S1566-0702(15)00291-X/abstract
“a subgroup of patients with POTS and joint hypermobility syndrome (JHS) has an underlying small fiber neuropathy and a reduction in Collagen IV in the basement membranes and blood vessels in the skin.” - Approximately 40% of Fibromyalgia cases have small fiber neuropathy
Fibromyalgia – Further Elucidation of Small Fiber Neuropathy Presence.
http://painmuse.org/?p=3178 - A subgroup of Fibromyalgia cases have frank Chronic Demyelinating Inflammatory Polyneuropathy (CIDP) – EMG findings, absent ankle jerks and high protein in CSP are features. IV immunoglobulins, pulse steroids, and plasmaphoresis can help:
Caro, X. J., Winter, E. F., & Dumas, A. J. (2008).
A subset of fibromyalgia patients have findings suggestive of chronic inflammatory demyelinating polyneuropathy and appear to respond to IVIg.
Rheumatology, 47(2), 208-211.
http://rheumatology.oxfordjournals.org/content/47/2/208.full.pdf+html
“Fifteen FMS/CIDP subjects were subsequently treated with IVIg (400 mg/kg each day for 5 days). Pain (P=0.01), tenderness (P=0.001) and strength (P=0.04) improved significantly. Fatigue and stiffness trended towards improvement.” - In children with widespread pain, POTS is typical, and gamma globulins and pulse steroids help
Fibromyalgia- Like Pains in Children Often a Treatable Small Fiber Neuropathy
http://painmuse.org/?p=2442 -
A case study of a 4-year-old girl with right leg CRPS “and dysautonomia (gastroparesis, postural tachycardia) refractory to multiple therapies, successfullytreated with therapeutic plasma exchange (TPE) with albumin replacement” – highlights autoimmune nature
Hendrickson, Jeanne E., et al.
Complex regional pain syndrome and dysautonomia in a 14‐year‐old girl responsive to therapeutic plasma exchange.
Journal of clinical apheresis 31.4 (2016): 368-374.
https://rsds.org/wp-content/uploads/2015/06/2015-CRPS-Dysautonomia.pdf -
“34.9% [of POTS] had significant adrenergic impairment, indicating that at least half of the patients had a neuropathic pattern of POTS.”
Thieben MJ, Sandroni P, Sletten DM, et al.
Postural orthostatic tachycardia syndrome: The Mayo Clinic experience.
Mayo ClinicProc 2007; 82: 308–313
https://s3.amazonaws.com/academia.edu.documents/45729387/82.3.30820160517-6955-iqrk33.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1523146130&Signature=fW5PnUOeOfiZD3OVx9B6sc%2BfzvM%3D&response-content-disposition=inline%3B%20filename%3DPostural_orthostatic_tachycardia_syndrom.pdf - In POTS autoimmmune antibodies are often (31/100+ cases) seen and 1/5 have an actual immune disorder
Blitshteyn, S.
Autoimmune markers and autoimmune disorders in patients with postural tachycardia syndrome (POTS).
Lupus 24.13 (2015): 1364-1369.
http://journals.sagepub.com/doi/abs/10.1177/0961203315587566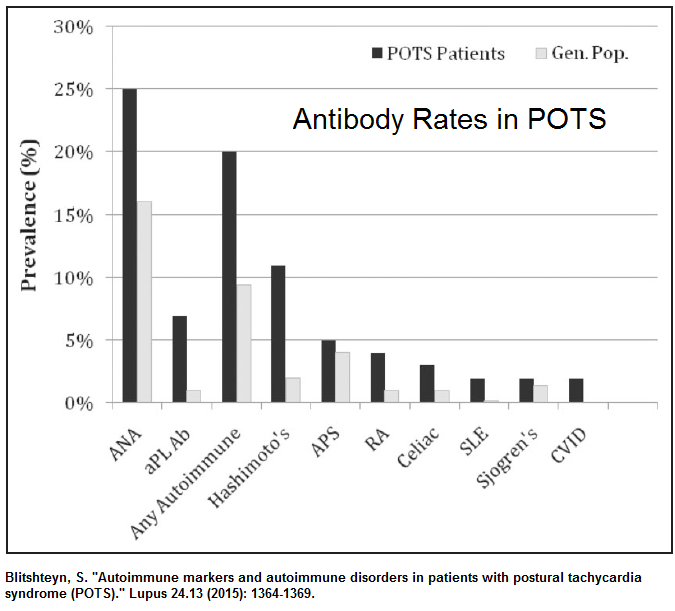 – 1/4 – positive ANA
– 1/4 – positive ANA
– 1/9 – Hashimoto’s thyroiditis ( with Thyroid antibodies)
– 4% celiac positive tissue transglutaminase antibodies ( does not include those with non-celiac gluten sensitivity)
– 7/100 had one elevated aPL ( antiphospholipid antibodies) and 5/100 had full features of anti-phospolipid syndrome
– 3/100 had Anti-SSB Ab: anti-Sjogren’s-syndrome related
antigen ; none had Anti-SSA – with 2/100 having Sjogren’s syndrome
– 4/100 had positive RA factor
– one had elevated anti-dsDNA Ab and one had atypical ANCA
– though not strictly autoimmune, “two patients had common variable immunodeficiency (CVID)” – immunoglobulin studies would show low IgA. IgG and maybe IgM - an array of autoantibodies against cardiac lipid raft microdomain proteins are present in patients with POTS that could effect cardiac function:
Wang, Xiao-Li, et al.
Autoimmunoreactive IgGs against cardiac lipid raft-associated proteins in patients with postural orthostatic tachycardia syndrome.
Translational Research 162.1 (2013): 34-44.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3691285/ - exposure to hidden antigens following cardiac ablation can trigger it:
Kanjwal K, Karabin B, Sheikh M, et al.
New onset postural orthostatic tachycardia syndrome following ablation of AVnode reentrant tachycardia.
J Interv Card Electrophysiol.2010;29:53 – 56
https://s3.amazonaws.com/academia.edu.documents/45264021/New_onset_postural_orthostatic_tachycard20160501-10914-130cylu.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1523289557&Signature=CKUQh%2FUrApLkvd36qBo6eCjBnbo%3D&response-content-disposition=inline%3B%20filename%3DNew_onset_postural_orthostatic_tachycard.pdfCholinergic Antibodies studies have now accumulated – these receptros are mediated by acetylcholine and are of 2 types – muscuranic (mAChR) and nicotinic (nAChR). Some of those with mostly nicotinic receptor antibodies has symptoms restricted to sicca syndrome(dry mouth and eyes), GI symptoms, and neurogenic bladder. Rest had panautonomic features.
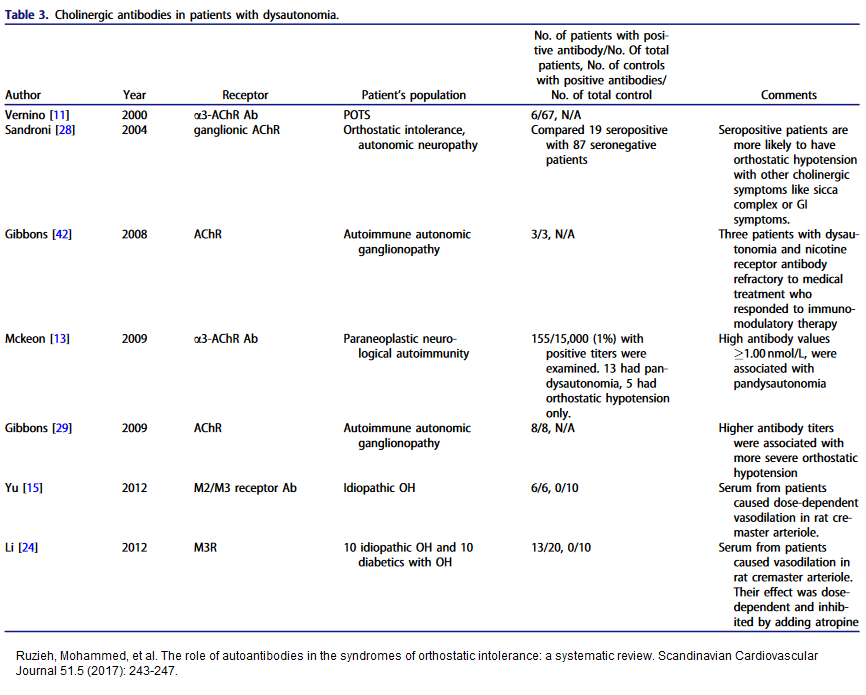
- In a Mayo Ckinic study, 6/42 = 10% POTS cases had a positive ganglionic acetylcholine receptor antibody (AChR antibody) perhaps similar to myasthenia gravis
Thieben MJ, Sandroni P, Sletten DM, et al.
Postural orthostatic tachycardia syndrome: The Mayo Clinic experience.
Mayo ClinicProc 2007; 82: 308–313
https://s3.amazonaws.com/academia.edu.documents/45729387/82.3.30820160517-6955-iqrk33.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1523146130&Signature=fW5PnUOeOfiZD3OVx9B6sc%2BfzvM%3D&response-content-disposition=inline%3B%20filename%3DPostural_orthostatic_tachycardia_syndrom.pdf - Ruzieh et al queried whether “For instance, it would be useful to know if
patients with ganglionic receptor antibodies experience more muscle weakness that may be treated with Pyridostigmine compared to their counterparts without these antibodies”. Indeed, that was tried and found beneficial:
Circulation. 2005 May 31;111(21):2734-40.
Acetylcholinesterase inhibition improves tachycardia in postural tachycardia
syndrome.
Raj SR(1), Black BK, Biaggioni I, Harris PA, Robertson D.
http://circ.ahajournals.org/content/111/21/2734.longHowever, use of pyridostigmine in fibromayglia failed to help pain and fatigue, though improvements in sleep and anxiety were thought due to improved vagal tone;
Jones, K. D., et al.
A six‐month randomized controlled trial of exercise and pyridostigmine in the treatment of fibromyalgia.
Arthritis & Rheumatology 58.2 (2008): 612-622.
https://onlinelibrary.wiley.com/doi/full/10.1002/art.23203 - antibodies to alpha 1 adrenergic receptors and beta 1 and
2 adrenergic receptors were found in 14/14 patients with POTS and not in controls
Li H, Yu X, Liles C, et al.
Autoimmune basis for postural tachycardia syndrome.
J Am Heart Assoc 2014; 3: e000755.
http://jaha.ahajournals.org/content/3/1/e000755.long
“Conclusions POTS patients have elevated α1AR autoantibodies exerting a partial peripheral antagonist effect resulting in a compensatory sympathoneural activation of α1AR for vasoconstriction and concurrent βAR-mediated tachycardia. Coexisting β1AR and β2AR agonistic autoantibodies facilitate this tachycardia. These findings may explain the increased standing plasma norepinephrine and excessive tachycardia observed in many POTS patients.” - This was confirmed in study that found “Eight, 11, and 12 of the 17 POTS patients possessed autoantibodies that activated α1AR, β1AR and β2AR, respectively.”
Fedorowski, Artur, et al.
Antiadrenergic autoimmunity in postural tachycardia syndrome.”
Ep Europace 19.7 (2016): 1211-1219.
https://academic.oup.com/europace/article/19/7/1211/2952372
supporting idea that “shifts in the α1AR and β1AR responsiveness are important in the pathophysiology of postural tachycardia”
adrenergic functions include:
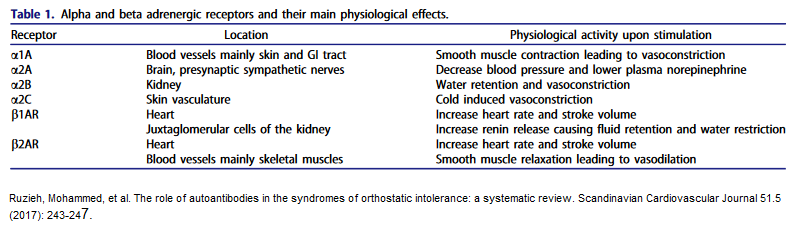 studies showing andrenergic antibodies in POTS have accumulated in last 6 years:
studies showing andrenergic antibodies in POTS have accumulated in last 6 years: - Endophin system pain suppression come in part through the Beta-adrenergic system:
Neurobiol Dis. 2013 Dec;60:39-50.
Antidepressants suppress neuropathic pain by a peripheral β2-adrenoceptor mediated anti-TNFα mechanism.
Bohren Y, Tessier LH, Megat S, Petitjean H, Hugel S, Daniel D, Kremer M, Fournel S, Hein L, Schlichter R, Freund-Mercier MJ, Yalcin I, Barrot M.
http://www.ncbi.nlm.nih.gov/pubmed/23978467
My summize – which if blocked by auto-antibodies is going to blunt descending pain inhibitition and increase pain. - Ruzieh (below) queried “whether patients with b1/b2-adrenergic receptors antibodies demonstrate more tachycardia responsive to Beta-blockers.”
-
In patients with above cholinergic receptor antibodies, higher titers correlate with the disease severity:
Ruzieh, Mohammed, et al.
The role of autoantibodies in the syndromes of orthostatic intolerance: a systematic review.
Scandinavian Cardiovascular Journal 51.5 (2017): 243-247.
https://www.researchgate.net/profile/Blair_Grubb/publication/318678950_The_role_of_autoantibodies_in_the_syndromes_of_orthostatic_intolerance_a_systematic_review/links/59cb8a73aca272bb050c24b2/The-role-of-autoantibodies-in-the-syndromes-of-orthostatic-intolerance-a-systematic-review.pdf - Growing concern of a POTS syndrome developing after papillomavirus vacinnation thought antoimmune in nature:
Blitshteyn, Svetlana, and Jill Brook.
Postural tachycardia syndrome (POTS) with anti-NMDA receptor antibodies after human papillomavirus vaccination.
Immunologic research 65.1 (2017): 282-284.
https://link.springer.com/article/10.1007/s12026-016-8855-1Butts, Breann N., Philip R. Fischer, and Kenneth J. Mack.
Human papillomavirus vaccine and postural orthostatic tachycardia syndrome: a review of current literature.
Journal of child neurology 32.11 (2017): 956-965.
http://journals.sagepub.com/doi/abs/10.1177/0883073817718731 - The situation is even getting more complex with vascular inflammatory markers being found in POTS:
Johansson, Madeleine, et al.
Inflammatory biomarker profiling in classical orthostatic hypotension: Insights from the SYSTEMA cohort.
International journal of cardiology 259 (2018): 192-197.
https://www.researchgate.net/profile/Fabrizio_Ricci3/publication/322936755_Inflammatory_biomarker_profiling_in_classical_orthostatic_hypotension_Insights_from_the_SYSTEMA_cohort/links/5a786d9445851541ce5b5f30/Inflammatory-biomarker-profiling-in-classical-orthostatic-hypotension-Insights-from-the-SYSTEMA-cohort.pdf
Summary – Autoimmune features are common in both POTS and Fibromyalgia. More severe forms and childhood versions can respond to IV gamma globulin, plasmaphoresis and maybe pulse steroids. The question is, which milder version would too. When would later mentioned antibody tests become available?
Association of a case of POTS with Chairi malformation brings up association of certain FM cases with treatable chairi syndrome cases. Our MRI testing is either unavailable or untrustworthy.
- A subgroup of fibromyalgia was found to have chairi malformation and found to benefit from surgery;
Eur Spine J. 2004 Oct;13(6):516-23. Epub 2004 Apr 9.
Clinical evidence for cervical myelopathy due to Chiari malformation and spinal stenosis in a non-randomized group of patients with the diagnosis of fibromyalgia.
Heffez DS, Ross RE, Shade-Zeldow Y, Kostas K, Shah S, Gottschalk R, Elias DA, Shepard A, Leurgans SE, Moore
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3476600/Eur Spine J. 2007 Sep;16(9):1423-33
Treatment of cervical myelopathy in patients with the fibromyalgia syndrome: outcomes and implications.
Heffez DS, Ross RE, Shade-Zeldow Y, Kostas K, Morrissey M, Elias DA, Shepard A
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2200733/pdf/586_2007_Article_366.pdf - Chairi syndrome was seen in a POTS case:
Prilipko, O., et al.
Orthostatic intolerance and syncope associated with Chiari type I malformation.
Journal of Neurology, Neurosurgery & Psychiatry 76.7 (2005): 1034-1036.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1739720/pdf/v076p01034.pdf
I had a case undiagnosable here, but seen on the same (though thought blurred) MRI images, diagnosable in the States. Makes me think our machines and image taking are inferior here, and competence in seeing certain cases of chairi, is a specialty feature.
Hypermobility association
Large association of POTS with Ehlers-Danlos hypermobility syndrome makes pain issues much more likely. Saw one case of CRPS caused by superficial radial nerve injury from unstable distal radius. Does one dare try prolotherapy to an already painful site?
Clin Orthop Relat Res. 2015 Feb;473(2):722-8.
doi: 10.1007/s11999-014-3898-x
Postural orthostatic tachycardia syndrome (POTS): association with Ehlers-Danlos
syndrome and orthopaedic considerations.
Grigoriou E et al
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4294907/pdf/11999_2014_Article_3898.pdf
Makes some interesting comments on POTS:
- “Large series have shown that a viral illness or surgical procedure can act as
triggering factors [12,20].”
Low, P. A., Opfer-Gehrking, T. L., Textor, S. C., Benarroch, E. E., Shen, W. K., Schondorf, R., … & Rummans, T. A. (1995). Postural tachycardia syndrome (POTS). Neurology, 45(4 Suppl 5), S19-25.
Thieben MJ, Sandroni P, Sletten DM, Benrud-Larson LM, Fealey
RD, Vernino S, Lennon VA, Shen WK, Low PA.
Postural orthostatic tachycardia syndrome: the Mayo clinic experience.
Mayo Clin Proc.2007;82:308–313
https://s3.amazonaws.com/academia.edu.documents/45729387/82.3.30820160517-6955-iqrk33.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1523817875&Signature=DdVN6Y79rQtXhbHOHWYYyZj0qAU%3D&response-content-disposition=inline%3B%20filename%3DPostural_orthostatic_tachycardia_syndrom.pdf - “In adults it can be an isolated syndrome or associated with porphyria, diabetes
mellitus, and paraneoplastic processes” - “children it tends to be an isolated syndrome with reports of spontaneous
resolution in approximately 75% of the patients by the age of 21 to 25 years” - “In a study by Gazit et al. [7], 80%of patients with joint hypermobility syndrome displayed symptoms of dysautonomia with orthostatic hypotension or POTS.”
Gazit Y, Nahir AM, Grahame R, Jacob G. Dysautonomia in the joint hypermobility syndrome. Am J Med. 2003;115:33–40. - Makes a warning re Florinef “Fludrocortisone, a mainstay salt-sparing
corticosteroid used in these patients, can cause, in higher
doses, significant hypokalemia and hypomagnesemia ” – and at higher doses risk of hip osteonecrosis (so stay low)
Low Serotonin – High Suicide Risk
Body- wide serotonin in POTS is low and POTS is associated with high suicide risk, adding a deeply troubling challenge to pain in POTS cases.
- One of the key places serotonin is stored is in platelet granules – in POTS there is a lack of these granules:
Gunning III, William T., et al.
Postural orthostatic tachycardia syndrome is associated with platelet storage pool deficiency.
Medicine 95.37 (2016).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5402587/ - low serotonin would suggest a depressive situation, and indeed there is a high suicidal risk in POTS syndrome:
Clin Auton Res. 2017 Apr;27(2):75-81.
doi: 10.1007/s10286-017-0399-5.
Health-related quality of life and suicide risk in postural tachycardia syndrome.
Pederson CL et al
https://link.springer.com/article/10.1007/s10286-017-0399-5
“Nearly half of our sample with POTS was at high risk for suicide”
they make the point that they often have poor physical health and stamina - In Fibromyaglia, there is a high Bipolar rate – varying from 20-26% on 2 surveys.
- In my ketamine trial, severe depressions accompanied some cases and milder version in other such that mood issues were involved in 80% of cases
- A serotonin stimulant antidepressant sertraline was tolerated though didn’t help POTS much but should be used re depression
J Psychopharmacol. 2014 Feb;28(2):155-61.
doi: 10.1177/0269881113512911.
Acute hemodynamic effects of a selective serotonin reuptake inhibitor in postural
tachycardia syndrome: a randomized, crossover trial.
Mar PL et al
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3956655/
Sleep Apnea
|Treatment of associated sleep apnea with CPAP may be complicated. Ordinary CPAP might not work and BIPAP might need to be tried. The anxiety that is associated might limit mask use and in one case, clonazepam 1 mg hs had to be used to reduce nightmares and ensure CPAP use.
- Sleep apnea can be one of the triggers in CRPS
Identification and Treatment of New Inflammatory Triggers for Complex Regional Pain Syndrome: Small Intestinal Bacterial Overgrowth and Obstructive Sleep Apnea
Weinstock, Leonard B. MD, FACG; Myers, Trisha L. PA-C; Walters, Arthur S. MD; Schwartz, Oscar A. MD; Younger, Jarred W. PhD; Chopra, Pradeep J. MD; Guarino, Anthony H. MD
A&A Case Reports: May 1st, 2016 – Volume 6 – Issue 9 – p 272–276
doi: 10.1213/XAA.0000000000000292
https://journals.lww.com/aacr/Fulltext/2016/05010/Identification_and_Treatment_of_New_Inflammatory.3.aspx
-ordinary CPAP was ineffective and patient was started on ” bilevel positive airway pressure (BiPAP) titration was completed with optimal settings of 15/11 with a nasal mask.”
-Patient would not keep mask on so required “clonazepam (1 mg/night) to reduce nightmares and reduce the urge to remove the BiPAP device.” - However, actual incidence of sleep apneain POTS is less than normal:
Miglis, Mitchell, Srikanth Muppidi, and Safwan Jaradeh.
Sleep Disorders in Patients with Postural Tachycardia Syndrome (P1. 279).” Neurology 84.14 Supplement (2015): P1-279.
http://n.neurology.org/content/84/14_Supplement/P1.279.short
However ” POTS patients reported greater difficulty falling and staying asleep, which was confirmed by polysomnography.”
Bacterial Overgrowth
It has been suggested that “gastrointestinal dysbiosis” can trigger mitochondrial dysfunction, microglial activation, and neuroinflammation seen in fibromyalgia and CRPS.
Vasquez, Alex.
Neuroinflammation in fibromyalgia and CRPS is multifactorial.
Nature Reviews Rheumatology 12.4 (2016): 242.
http://www.autoimmunity-network.com/media/moxie/files/a/ad/adm/admin/VASQUEZ_2016_NeuroinflammationPain.pdf
Cases are found of POTS helped by treatment of bacterial overgrowth.
Weinstock, Leonard B., et al.
Successful treatment of postural orthostatic tachycardia and mast cell activation syndromes using naltrexone, immunoglobulin and antibiotic treatment.
BMJ case reports 2018 (2018): bcr-2017.
http://casereports.bmj.com/content/2018/bcr-2017-221405.full.pdf
Bacterial overgrowth could also explain why Cefadroxil antibiotic cured one CRPS case:
Ware, Mark A., and Gary J. Bennett.
Case report: long-standing complex regional pain syndrome relieved by a cephalosporin antibiotic.
PAIN® 155.7 (2014): 1412-1415.
http://pedroschestatsky.com.br/_files/view.php/download/material/92/547ca1ae40060.pdf
Need to add here but article has become never ending…
Situation gets more complex with the association of pain, mast cell disease, and POTS (with abnormal tilt test)recently documented
Association of chronic pain and abnormal tilt table test with tryptase metabolism abnormality:
Lyons, Jonathan J., et al.
Elevated basal serum tryptase identifies a multisystem disorder associated with increased TPSAB1 copy number.
Nature genetics 48.12 (2016): 1564.
http://europepmc.org/articles/pmc5397297
Clinical features and gene-dose effects in hereditary α-tryptasemia syndrome: IBS = irritable bowel syndrome; COMPASS31 – mentioned in intro as an autonomic function questionnaire
| Hereditary α-tryptasemia syndrome (α) | TPSAB1 duplication (αα) | TPSAB1 triplication (ααα) | P valuea | ||||
| Serum tryptase, ng/ml Median Interquartile range | 15.9 12.6–20.7 |
14.3 11.6–17.8 |
23.4 19.8–26.4 |
<0.0001 | |||
| Manifestation | n | % | n | % | n | % | P valuea |
| Systemic venom reactionb | 15/96 | 16 | 11/73 | 15 | 4/15 | 27 | NS |
| Flushing/pruritus | 49/96 | 51 | 33/73 | 45 | 12/15 | 80 | 0.022 |
| IBS (Rome III) | 34/70 | 49 | 26/53 | 49 | 7/12 | 58 | NS |
| Chronic gastroesophageal reflux symptoms | 62/96 | 65 | 42/73 | 49 | 15/15 | 100 | 0.001 |
| Congenital skeletal abnormalityc | 25/96 | 26 | 14/73 | 19 | 8/15 | 53 | 0.009 |
| Retained primary dentition | 20/96 | 21 | 12/73 | 16 | 7/15 | 47 | 0.016 |
| Hypermobility (Beighton score ≥4)d | 14/50 | 28 | 11/30 | 37 | 3/13 | 23 | NS |
| COMPASS 31e | 33/70 | 47 | 26/57 | 46 | 5/11 | 45 | NS |
| Positive tilt-table test | 11 | ≥11 | 6 | ≥8 | 4 | ≥26 | ND |
| Arthralgia | 43/96 | 45 | 31/73 | 42 | 11/15 | 73 | 0.045 |
| Body pain/headache | 45/96 | 47 | 32/73 | 44 | 11/15 | 73 | 0.049 |
| Sleep disruption | 37/96 | 39 | 23/73 | 32 | 11/15 | 73 | 0.004 |
As mentioned earlier, POTS with mast cell activating syndrome and POTS was successfully treated in part with a glial modifier, Naltrexone – part opioid,
Weinstock, Leonard B., et al.
Successful treatment of postural orthostatic tachycardia and mast cell activation syndromes using naltrexone, immunoglobulin and antibiotic treatment.
BMJ case reports 2018 (2018): bcr-2017.
http://casereports.bmj.com/content/2018/bcr-2017-221405.full.pdf
they used only 1 mg /day(“as opposed to ideal dose of 4.5 mg”- for financial reasons).
“Ultra-low-dose naltrexone for 6 weeks improved body pain, mood, memory, sleep, flushing, food and odour sensitivities and paraesthesia: 7% decrease in POTS and 17% decrease in MCAS severity scores.”
studies have suggested use in CRPS:
Chopra, Pradeep, and Mark S. Cooper.
Treatment of complex regional pain syndrome (CRPS) using low dose naltrexone (LDN).
Journal of Neuroimmune Pharmacology 8.3 (2013): 470-476.
https://link.springer.com/article/10.1007/s11481-013-9451-y
- narrows down the issue t0: “During neuroimmune activation, TLR4 (Toll-Like Receptor 4) is upregulated in microglia” – “This correlates with the rodent developing neuropathic pain”. TLR4 “augments the production of pronflammatory cytokines via the NF-κB pathway”. Naltrexone is a TLR4 antagonist and works to suppress neuropathic pain in the rat model. Naltrexone may help Fibromyaglia pain.
Unfortunately, not practical for those already on opioids
Rarely, deficiencies can help POTS:
B1-Thiamine
Blitshteyn, Svetlana.
Vitamin B1 deficiency in patients with postural tachycardia syndrome (POTS). Neurological research 39.8 (2017): 685-688.
https://www.tandfonline.com/doi/abs/10.1080/01616412.2017.1331895
6% had vitamin B1 deficiency, and one of four deficient patients experienced significant improvement of POTS after oral vitamin B1 supplementation. (B1 100 mg/day)
Vitamin D
Chaudhari, Shilpa Abhay, Alan Sacerdote, and Gul Bahtiyar. “1-α hydroxylation defect in postural orthostatic tachycardia syndrome: remission with calcitriol supplementation.” BMJ case reports 2012 (2012): bcr0220125730.
http://europepmc.org/articles/pmc3433525
Maybe Iron
Antiel, Ryan M., et al. “Iron insufficiency and hypovitaminosis D in adolescents with chronic fatigue and orthostatic intolerance.” Southern medical journal 104.8 (2011): 609-611.
https://www.ncbi.nlm.nih.gov/pubmed/21886073
Just state deficiencies are common – not that supplementation helped
?Choline
Schenkel, Laila C., et al. “Mechanism of choline deficiency and membrane alteration in postural orthostatic tachycardia syndrome primary skin fibroblasts.” The FASEB Journal 29.5 (2015): 1663-1675.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4415014/
- choline involved in lipid homeostasis, and mitochondria function which involved in tissue samples of a deficient case
Comments – this is a huge field that is just beginning to become clear. It is clear many avenues need to be pursued in treatment of this symptom complex. Antidepressants may be indicated for both serotonin effects and mood. Rarely occurring deficiencies, sleep disorders, and bacterial overgrowth treatment might help. More severe cases may need steroid pulses, pulse immunoglobulins, and plasmaphoresis. Association with mast cell syndromes needs attention.
there is a site that ddscribes non- drug treatment measures in detail: (last half of page)
https://www.dinet.org/content/information-resources/pots/pots-what-helps-r100/
in case it goes down, I have a word version:
pots measures