
The most successful treatment for CRPS especially early is Prednisone. It is even used in wrist fracture situation. Yet this fact seems not all that well known as is the fact one should continue the course for 8 weeks. Needless suffering though ignorance.
Winston, Paul et al
Early treatment of acute complex regional pain syndrome after fracture or injury with prednisone: why is there a failure to treat? A case series.
Pain Research and Management 2016 (2016).
http://dx.doi.org/10.1155/2016/7019196
http://downloads.hindawi.com/journals/prm/2016/7019196.pdf
How can you tell a wrist fracture is going to be a problem? – You can look for the fancy signs like change in temperature, skin sensitivity and so on but the basic fact is “it hurt’s like hell” – If the pain is outside what one would expect in a wrist fracture then treat as CRPS- as per
Moseley, G. Lorimer, et al. “Intense pain soon after wrist fracture strongly predicts who will develop complex regional pain syndrome: prospective cohort study.” The Journal of Pain 15.1 (2014): 16-23.
https://cdn.bodyinmind.org/wp-content/uploads/1-s2.0-S1526590013012017-main.pdf
- “widespread use of prednisone likely remains low, potentially resulting in long-term pain, joint contracture, and disability.”
“After fracture, rapid recognition and treatment with prednisone
may alter the course of this process and prevent significant disability” - One of the reasons would be the fact that a randomized control trial has not been done likely because it would be UNETHICAL to do so given its effectiveness. Hence Cochrane won’t comment on its effectiveness earning Cochrane’s place in being one of “Voltaire’s Bastards” ( a Canadian book on rationalism being unethical- where evidence based medicine is a bastard…)
- This article states “This readily available treatment shows efficacy within days of treatment“
- They present 3 cases with rapid resolution with prednisone. Their protocol uses 60 mg initially – going down by 5 mg each day until 20 mg reached and staying on 20 mg until symptoms subside – which is within 1 month. (read later how 2 months is better)
Some studies of Prednisone use:
D. F. Braus, J. K. Krauss, and J. Strobel
The shoulder-hand syndrome after stroke: a prospective clinical trial
Annals of Neurology, vol. 36, no. 5, pp. 728–733, 1994.
https://onlinelibrary.wiley.com/doi/abs/10.1002/ana.410360507
- “31 of the 36 patients became almost symptom free within 10 days’ treatment with low doses of oral corticosteroids.”
Bianchi, C., et al.
Long-term functional outcome measures in corticosteroid-treated complex regional pain syndrome.
Europa medicophysica 42.2 (2006): 103-111.
http://europepmc.org/abstract/med/16767061
- 26/31 due to fracture
- “40mg to 60mg of prednisone and titrated over several weeks”
- improvements persisted at one year
N. S. Atalay, O. Ercidogan, N. Akkaya, and F. Sahin,
Prednisolone in complex regional pain syndrome
Pain Physician, vol. 17, no. 2, pp. 179–185, 2014.
https://www.researchgate.net/profile/Fusun_Sahin/publication/261034135_Prednisolone_in_Complex_Regional_Pain_Syndrome/links/55dad0f008aeb38e8a8a2268.pdf
- 45 cases with upper extremity CRPS mean age 43
- dose of 30 mg Prednisolone (equivalent dose for prednisone) and tapered by 5 mg every 3 days until discontinuation after 3 weeks (I think that was suboptimal dose)
- pain dropped from 3.5/10 to 1.2/10 after 3 weeks
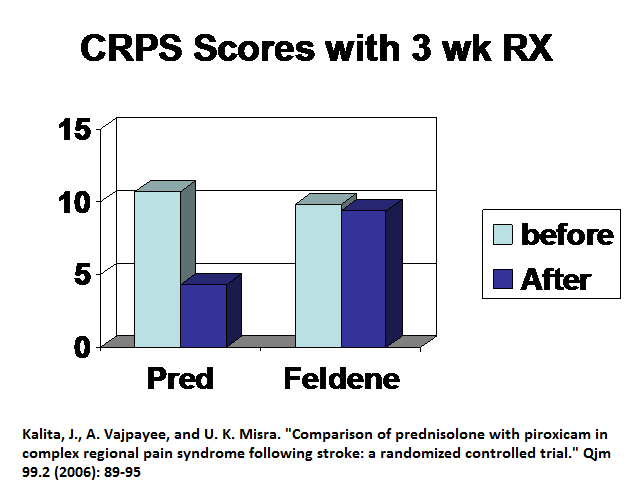
Comparison of prednisolone with piroxicam in complex regional pain syndrome following stroke: a randomized controlled trial
J. Kalita A. Vajpayee U.K. Misra
QJM: An International Journal of Medicine, Volume 99, Issue 2, 1 February 2006, 89–95
https://doi.org/10.1093/qjmed/hcl004
https://watermark.silverchair.com/hcl004.pdf?token=AQECAHi208BE49Ooan9kkhW_Ercy7Dm3ZL_9Cf3qfKAc485ysgAAAaMwggGfBgkqhkiG9w0BBwagggGQMIIBjAIBADCCAYUGCSqGSIb3DQEHATAeBglghkgBZQMEAS4wEQQM5qnhJ_n_M3Q0snBNAgEQgIIBVjCO6PfjWM77Ddsk-CZe-MyC-aO_rDUjaVlSFgQuM2Fb9GMZs-1xEDAt5vcnVVfj2yNXprtsGMfVKzS5b2NCjV2OSj5e80oYXDl8-JkW9o9eYwJCJPwFv1uAc_Y13GHbIknT6Vy6VnqNst0FZEkYOowd2TMoiWpcMUjdFnOtqMi0GUUu2qLyLK4SU6NAY4-iuApzF4jxAl6tQnmBbQpptiqfM9cBToCoiSw_Cz3XV9BnQ0_1xc6TmMkgaBJCGfVV8xBy4gICG0fY9vApY9c1kXqytC6rtrLQa_tI2dnYQxhDsmG9ox_OqNkFgOXoUOru2b7visSHIURqzt5Ogi3bfT4sdGD8BfK0hycqSjxJAQrH9fTCdzaLgOZwJ3gsYr-OPr6vow_GG-kz2ZRcfjH1cbG_ySxcJOoDVE4PCuoJrfKPpHWJnwlHnvqy10Sll6WznPZUpMiIKA
- CRPS following a stroke
- 60 cases average age 54
- Prednisone 10 mg tid or piroxicam (feldene) 20 mg od – (I believe prednisone dose still suboptimal)
 I contend with higher doses this could be lower.
I contend with higher doses this could be lower.
Part of that comes from a study of what Prednisolone doses ( prednisone would be equal doses) does for ankylosing spondylitis flares:
Ann Rheum Dis. 2014 Jan;73(1):243-6.
doi: 10.1136/annrheumdis-2012-203055.
Efficacy of oral prednisolone in active ankylosing spondylitis: results of adouble-blind, randomised, placebo-controlled short-term trial.
Haibel H et al
20 mg prednisolone – did NOTHING
50 mg – did well with 2 weeks
I would suggest that victims of CRPS should be treated with 2 wks of 50 mg prednisone daily . How long the treatment? – TWO MONTHS
Kalita, Jayantee, et al.
Long-term prednisolone in post-stroke complex regional pain syndrome.
Pain physician 19.8 (2016): 565-574.
http://www.painphysicianjournal.com/current/pdf?article=MzEwNA%3D%3D&journal=100
- 58 post stroke CRPS
- allocated to 2 week rx of 30 mg /day or 30 mg /days x2 weeks and taper over 6 weeks
results: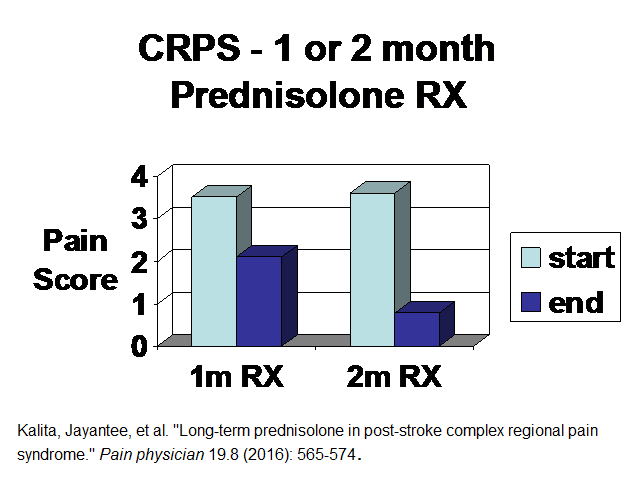 Comment – I recently treated a post wrist fracture CRPS :
Comment – I recently treated a post wrist fracture CRPS :
50 mg od prednisone for 2 weeks ( I routinely give alprazolam PRN sedative as some become quite activated with agitation and insomnia).
Tapered down from 50 mg to off over remaining 6 weeks – near the end she had minimal pain.
How does it work in longstanding CRPS – there was a stupid study done that did not about results of above study as it was not out yet.
Barbalinardo, Stefania, et al.
The treatment of longstanding complex regional pain syndrome with oral steroids.”
Pain Medicine 17.2 (2015): 337-343.
https://academic.oup.com/painmedicine/article/17/2/337/2460703
- 31 cases over 3 months not responding to treatment ( might not be representative being resistant cases)
two centres
- 100 mg prednisolone/day tapered by 25 mg every 4 days – so only 16 days RX
- 60 mg /day lowered every 4 days by 20 mg until off – so only 12 days treatment
Results – much as would be expected from study above found this one found – under two months treatment gains you suboptimal results and very little was found in their study. Can’t conclude much from it yet I am sure it will now become standard gospel that treating long term CRPS with steroids is ineffective. What a disappointment.
Comment – I would contend that after 3 months local issues become important and peri-neural njection to skin, Intramuscular stimulation to muscles, Botulinium to any dystonia, and steroid injections to radio-ulnar and radiohumeral joints will be important but I will write separately about those things. In longstanding cases, I would still use my protocol of prednisone but not expect results in first 2 weeks.
With 2 months of Prednisone one must be willing to accept the rare risk of osteonecrosis of hip where hip collapses and one needs a hip replacement….
Came across a CRPS article where it was stated:
“CRPS I was diagnosed. Treatment with regular stellate ganglion blockade and infra-red therapy was initiated. The therapy proved to be effective in relieving pain and hyperalgesia and in ameliorating the range of motion, although the effect was not long-lasting. Despite the treatment being continued for approximately 10 months, pain and oedema have now spread contralaterally to involve the right hand.”
I’m thinking “why were they too dumb to use prednisone early on?” Prednisone can be a game changer…