
Awe inspiring case of chronic migraine headaches eliminated by pulsed radiofrequency (low burn) to a neck sympathetic ganglion.
Carcamo, Cesar R.
Pulsed Radiofrequency of Superior Cervical Sympathetic Ganglion for Treatment of Refractory Migraine.
Pain Medicine 18.8 (2017): 1598-1600.
https://academic.oup.com/painmedicine/article/18/8/1598/2833958
- 24 year old with frequent drug-unresponsive migraine headaches
- “PRF lesioning was performed for a total of five cycles of 120 seconds each. The preset maximal temperature was 45 °C and 70 V using a NeuroTherm NT1,000 (NeuroTherm, Inc., Middleton, MA, USA) radiofrequency generator.”
- completely free of headaches for 10 month followup
- they felt “sympathetic block may involve a reduction in the neuroinflammatory process”
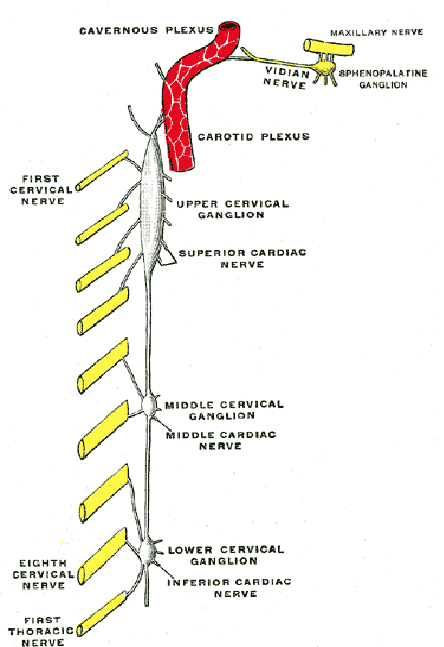
superior cervical ganglion is at level of c3 anterior to vertebral body and close to carotid artery
 article uses ultrasound monitoring to guide but it refers to another article:
article uses ultrasound monitoring to guide but it refers to another article:
Koning, Henk M., et al. Percutaneous radiofrequency lesion of the superior cervical sympathetic ganglion in non-traumatic neck pain.
The Pain Clinic 12.4 (2000): 271-279.
https://s3.amazonaws.com/academia.edu.documents/42121361/Percutaneous_radiofrequency_lesion_of_th20160205-30232-1ljes4y.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1522649321&Signature=kRKaj6bbZq7uRx2%2Bc2fgnjGq%2BDA%3D&response-content-disposition=inline%3B%20filename%3DPercutaneous_radiofrequency_lesion_of_th.pdf
they used xray imaging but gave better idea of how injected:
- entry point of the needle is chosen overly-ins the facetal column at the level of the third cervical vertebrae
- advanced until the tip is situated a few millimeters anterior to the anterior border of the vertebral bodies
- appears to be anterior to longus collis but below/ lateral to carotid carotid
- article radiofrequencied 100 cases of non-truamatic neck pain.
- most patients (93%) rated their pain intensity as serious or intolerable
- 6% had temporary worsening of pain lasting up to 2 months; “4% reported a change in sensibility in the painful region ” ?more tender or more numb??
- 1/2 got some relief and “two years after the treatment, the maintenance of pain relief occurred in eighty per cent of the patients responding to this therapy”
Comment – remarkable results but few trained to do this procedure; first article is from Chile. Going in over c3 facet is exactly where upper superficial cervical plexus lies and so you might end up going through it to get to this deeper ganglion. Hopefully more will be published on this subject as it sounds very promising.