I am sending out a call for people to help petition the government for coverage of pain medications in Saskatchewan. This is a letter I sent out through the Sask. Pain Network:
To Sask Pain Network:
It seems impossible to treat chronic pain in Saskatchewan. Many of the useful agents are NOT covered by the drug plan and never will be, because they do not demonstrate good effect as a “stand alone” treatment, and are not reliably responsive in groups that are of diverse causes. ( Ex. treating back pain only once with Botox will not hit all the necessary areas to show benefit and treating back pain with Botox may not help a facet and SI joint problem).
Dr. Theil (gynecologist),and I (separately) applied to the drug plan some years ago for coverage for Botox for pelvic pain. I submitted a report of about 20 pages, but got no response. It also seems clear that now the drug plan is more cash -strapped from covering seniors’ prescriptions. I feel nothing of value will ever be covered. People with chronic pain are generally too poor to handle much in the way of drug costs.
I discussed this with Dr. Murray Opdahl (Saskatoon Pain Clinic) and he is similarly frustrated by lack of access to useful treatments. Individually, we have been ignored. As a group, with knowledge in the area of pain, our voice would be one to be reckoned with. Some agents that have shown benefit in select cases include:
Botox as an adjunct to many problems. (~$400.00/bottle – could use 2+)
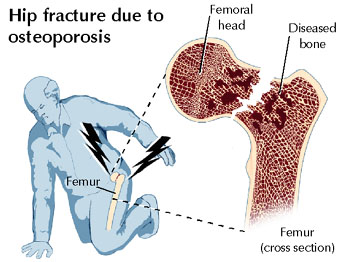
Pamidronate for Complex Regional Pain Syndrome (aka RSD), and post vertebral fracture ($400.00 x 2-3 for treatment)
Enbrel for radiculitis ( needs TWO shots – not like one one-shot failing remicade study) $250.00 X 2
Lyrica for – Fibromyalgia (recently gained formal approval in USA) and certain neuropathies ~ 150-200/month
Tramadol – especially for pain in elderly or those intolerant to other opioids $150+/month depending
Cymbalta for chronic pain with depression – $150+/month
There is more. We also need a pain clinic in Regina and Dr. Lang (Anesthesia) appears willing to run it (though obviously more multidisciplinary help would be needed).
I would invite all interested parties to submit here. ( I won’t publish your name online unless specifically requested or have comments you wish to make)