
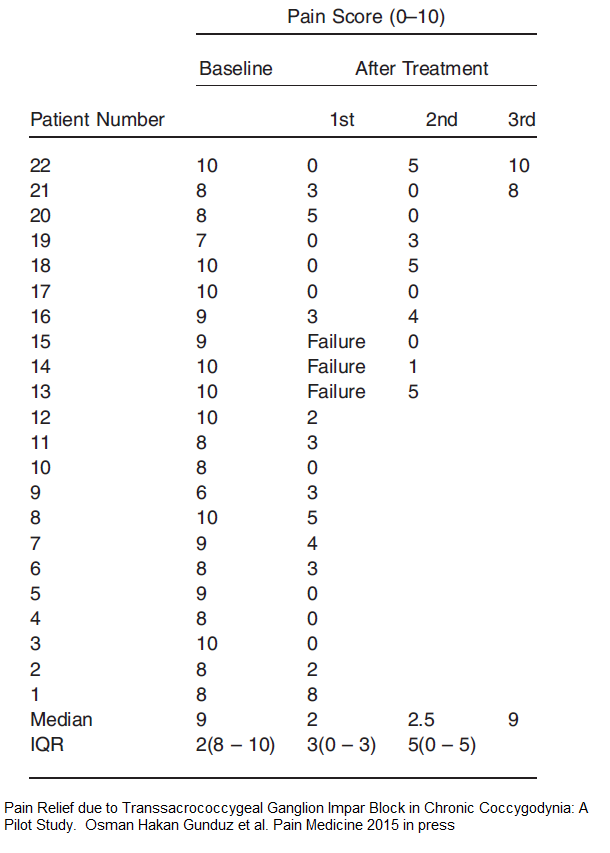
One Ganglion Impar injection achieved over 50% improvement for 82% of cases that lasted an average of 6 months.
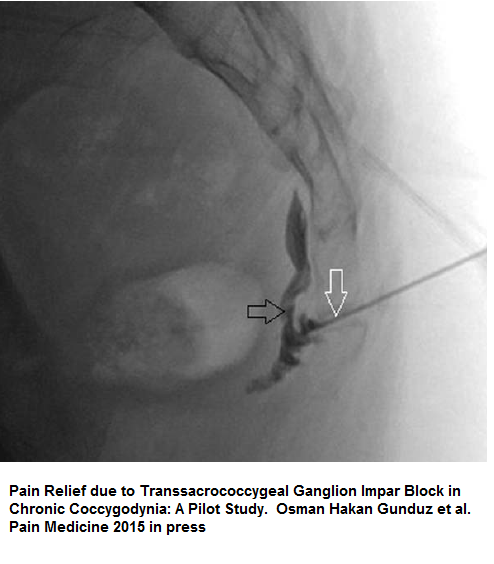
Pain Relief due to Transsacrococcygeal Ganglion Impar Block in Chronic Coccygodynia: A Pilot Study
Osman Hakan Gunduz, Savas Sencan, Ozge Kenis-Coskun.
Pain Medicine 2015 in press
http://onlinelibrary.wiley.com/doi/10.1111/pme.12752/abstract
- 22 cases not responding to conservative therapy
- fluoroscopy-guided transsacrococcygeal ganglion impar block – “With the patient lying prone, the sacrococcygeal joint was visualized via fluoroscopy. A 22-gauge spinal needle was used to reach the ganglion impar. After injection of contrast material and confirming the position of needle, 2 mL of 0.5% bupivacaine, 2 mL
saline, and 1 mL (40 mg) of methylprednisolone were injected in the area.” - Results were so good I included table here:
Comment – I have written on ganglion impar injections before:
Ganglion Impar Injection For Tailbone Coccydynia
http://painmuse.org/?p=1351
New Treatment of Perineal / Pelvic Pain – Botox to Ganglion Impar
http://painmuse.org/?p=334
Several observations:
- ganglion is more often 1 coccyx segment down from sacrococcygeal joint so injection there might be better
- Don’t need a spinal needle unless fat. In a thin lady I felt a 30 gauge needle just penetrate . 25 guage 1-1/4 inch might do unless significantly obese for many.
- If not using imaging, just put on cipro 1 gm/day for 3 days if rectal examining after shows blood
- I am however cannot responsible for individual cases where more care might be warranted.
- I have just used 5% lidocaine without steroid and that might be bit safer but probably needs repeating 3 times for good take.
Some other suggestions for coccyx are here:
New Treatments For Coccygodynia (sore Coccyx)
http://painmuse.org/?p=2073
I requested this injection; WCB Claim file information states; They couldn’t understand how this would help: Didn’t even know what it was, and would not even listen as they had already made their mind up, I would NEVER get better unless I realize the pain is not coming from my tailbone; 1 year later I was diagnosed with “Coccydynia” consequence of my slip / fall from the top of grain trailer and landing on my buttocks / back on the steel trailer frame. I was denied any help at Royal University Hospital by a doctor who deliberately sent a falsified report to WCB. (That’s a story for another day) Doctor #4 finally ordered an x-ray 1 week after injury; The radiologist wrote:
EXAMINATION:
COCCYX AND SACRUM:
History: Fell 1 week ago.
It is possible the coccyx is fractured at the level of the first coccygeal segment and tip of the sacrum but this is debatable. In any case further radiographic follow-up will not be necessary. The SI joints are symmetric. No abnormality is seen with the pubic rami or pubic symphysis.
Conclusion: Possible coccygeal fracture.
(11 years since injury and WCB is still debating:)
“Read this Injured Workers Appeal;” ( “It clearly identifies, MRI – CT Scan – Bone Scan and other diagnostic tests could NOT proper identify the severity of injury: ONLY after receiving surgery, was the severity of injury identified” )
https://www.canlii.org/en/bc/bcwcat/doc/2003/2003canlii70455/2003canlii70455.html?searchUrlHash=AAAAAQAKY29jY3lkeW5pYQAAAAAB&resultIndex=26
Please Note: This injured worker suffered workplace injury on January 1, 2000
“A second and third orthopaedic surgeon declined to perform surgery”
The worker saw a neurologist, who could not find any neurological reason for the worker’s ongoing chronic pain. In his report of October 16, 2001, the neurologist noted the worker seemed angry with him.
The fourth orthopaedic surgeon performed surgery on October 23, 2002. He found that the last segment of the coccyx was mobile, and he removed it. This did not improve the worker’s chronic pain situation, although he later stated that it slowed down the deterioration.
On November 27, 2006, another of the family doctors (at the same clinic) wrote a letter describing his involvement with the worker. He stated that the worker continued to be affected by severe, intractable, coccygeal pain which had a marked impact on his day‑to‑day activities. It made it difficult for him to sit, kept him awake at night, interfered with much of his physical activity, and interfered with his sex life. The worker was using narcotic medications. The doctor stated that the worker continued to be disabled by the injury.
The Injured worker had further appeal:
https://www.canlii.org/en/bc/bcwcat/doc/2008/2008canlii50181/2008canlii50181.html?searchUrlHash=AAAAAQAKY29jY3lkeW5pYQAAAAAB&resultIndex=12
—————————–
Bruce,
I find this scenario sickening. WCB case workers seem to operate under certain axioms:
1) If it not broken it can’t be bad. People are aware that instability in knee (eg torn anterior cruciate ligament) accelerates deterioration but are unwilling to suppose injury causes subtle instabilities and deterioration elsewhere. Torn and mild bulging disc can lead to sciatica without even touching a nerve root. I could go on.
2) If MRI/CT can’t see it, there can’t be any much pain.
3) Chronic pain should get better with time so you can automatically cut them off coverage when you feel like it.
None of these are true and a Canadian provincial Supreme court ruling has already accepted that chronic pain exist without objective evidence and has to be considered. WCB likes to forget about these rulings
4) If you can make rehab too painful to follow and they quit rehab – you can cut their coverage – while there has already been a WCB ruling stating a case can quit rehab and still be covered, cases worker have forgotten about that.
They also like to suppose if someone is susceptible to an injury, it is not their concern. However, the “thin skull rule” demands that their claim is as good as anyone’s.
Lastly, they like to assume a specialist would be a good judge of pain intensity and hence disability – while the opposite is true – “Experts” become jaded and cannot reliably predict pain severity – university freshmen are better predictors in one study.
The whole system is sick. Case workers have no interest in a case’s recovery – only in cost containment at all cost. Those that live by above axioms need to be fired – or retrained and have their work monitored. It would take political legislation to make these sort of changes. In our province, we have one of the lowest auto-insurance costs in North America – all due to the fact sick victims are terminated from coverage with rehab that does not work well. So we enjoy low insurance cost on the backs of these victims.
Where I live, worker’s advocate is impotent for lack of medical expertise to counter WBC medical assertions.
I’m so sorry.
-admin
Doc, our group of injured workers in Saskatchewan have been comparing claims; “We found, WCB in many claims, use the same 2 specialists for the 1-2 punch: First they send you to specialist #1 which of course refuses any investigation, and plays the “stereo-typical medical commentary, psychological card” – then WCB sends you to #2 specialist for a repeat of the previous scenario: Once this is done, your DOOMED: Any further physician won’t investigate as it would prove these 2 failed to actually due their job.
This summer we lost one of our members, “Stress Induced Heart Attack” courtesy WCB. His story was very unique, after suffering workplace injury he had a male case manager, who actually was treating him fairly: ( WCB turfed him, 6 months into the claim ) then the new case manager, rewrote his tertiary assessment, rewording it with
BS lies. Which resulted in the termination of WCB benefits. WCB won through attrition. We are being deliberately “MURDERED” by WCB: I don’t believe anyone can understand the EVIL unrelenting abuse injured workers are subjected to by WCB employees and their “Highly Paid Contract Doctors” who seem to enjoy selling out severely disabled injured workers, for their $REWARD$:
Hey Doc, recently the website,
https://www.hpiw.org/testimonials;
Was removed from the internet? Was this due to “Pressure” from Government, Workers Compensation? This following statement, made by Physician truly becomes a Injured Workers “Worst Nightmare”; ( “” In my practice these are not isolated cases. Rather than facilitate treatment, the WSIB’s behavior seems aimed at inflicting as much distress as possible on these very vulnerable people.”” ) Talk about hitting the proverbial “Nail on the Head!” In my Sask WCB Claims ” WCB Employees have deliberately “Falsified” my medical information, even taking another injured workers X-Ray Report / Specialist Report, then inserting this information into my WCB claim file and sending it to treating physicians, to make them believe, my workplace injury has been investigated, when it has deliberately been refused any investigation. On top of all this, when attempting to “Appeal decisions” WCB employees deliberately have repetitively entered “Falsified / Fictitious” lies, into “Summary Document” used for WCB Board Level Appeal’s. My request to WCB for copy of “Summary Document” prepared for Board Level Appeal – request for “Full Disclosure” – “Deliberately Denied” – ( only after obtaining Attorney did WCB release Summary Documents; ) “How can any injured worker receive a “Fair – Impartial – Honest” Appeal Hearing, with WCB Board Members, when Injured Worker is “deliberately denied FULL DISCLOSURE” of information in “Summary Document” used for “WCB Board Level Tribunal?”
“It Boggles the mind, to the extent WCB uses to “Deliberately Deny” Medical Investigation / Medical Treatments of workplace injuries;
Below is “Only Some” of what physicians have opinioned, with their experience with workers compensation. How is any severely injured worker able to have “ANY CHANCE” for health recovery from workplace injury, when WCB Employees, WCB Tribunals, go to “ANY LENGTHS” to DENY, medical investigations requested from physicians / specialists when “Non-Medical WCB Employees” violate Canadian criminal code, to prevent requested medical intervention?
What we’ve heard.
“A vulnerable population is being systematically re-injured. These injured workers end up traumatized by the system designed to help them, not only psychologically but financially, socially and in their family relationships.”
— PSYCHOLOGIST, NORTHERN ONTARIO
“I have many patients who are impacted negatively by their involvement with WSIB at a time when they are trying to heal. It is devastating to many that the organization that they believe to be their support becomes their adversary.”
— PSYCHOLOGIST, SOUTHERN ONTARIO
“My experience has been that most injured workers receive good services from the WSIB. However, I’m concerned that a minority of patients with complex injuries are falling through the cracks and in some cases being mistreated by a system that appears to prioritize cost-cutting over patient outcomes.”
— PHYSICIAN, GTA
“I have stopped accepting new WSIB clients due to continual frustrations working with WSIB. Premature return to work against medical and psychological advice, arbitrary termination of sessions, failure to advise regarding acceptance/denial of treatment plan/sessions, patients forced to take programs in Toronto offering treatments I was already providing. I did not want to collaborate with a system that was designed to fail patients.”
— PSYCHOLOGIST, KINGSTON
“Inappropriate “work hardening” programs where the effect of pain on physical/mental activity is ignored, hostile, adversarial nurses and adjudicators who deny even the most basic pain care, absurd assessments by physicians and other health professionals who have no understanding of chronic pain management and outright misrepresentation of workers’ problems have been the rule among the people I treat. WSIB personnel behave in an arbitrary fashion and seem unaccountable to anyone. In my practice these are not isolated cases. Rather than facilitate treatment, the WSIB’s behavior seems aimed at inflicting as much distress as possible on these very vulnerable people.”
— PHYSICIAN, CHRONIC PAIN SPECIALIST, GTA
“I hate to see injured workers suffer and have to deal with delays and denials, and to have their experiences discounted in their on-going efforts to receive appropriate and timely support. Of course, this is also a huge frustration and deterrent to wanting to work with this population, because as a professional it is really hard and really time consuming to continue to fight!”
— PSYCHOLOGIST, GTA
“Too often I have seen injured patients subjected to inhumane treatment by the WSIB machine. Cleverly disguised professionals add their weight to further harm the injured worker. This has to stop.”
— CHIROPRACTOR, NORTHERN ONTARIO