
6-8 years ago a brief neuralgic pain in the scalp that radiated to front or back of head was described. I wrote about it here:
http://painmuse.org/?p=1516
Now a facially originated version has been defined and sounds very much like trigeminal neuralgia except it shots up or down the face. The same superior cerebral artery compression was found on MRI as you see in Trigeminal neuralgia.
Cephalalgia. 2016 Sep 6. pii: 0333102416668656. [Epub ahead of print]
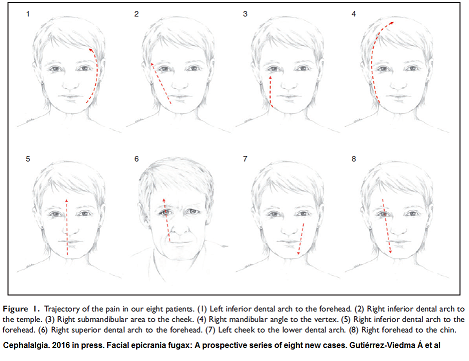
Facial epicrania fugax: A prospective series of eight new cases.
Gutiérrez-Viedma Á et al.
http://www.ncbi.nlm.nih.gov/pubmed/27605570
- 8 cases unilateral paroxysms
- 6 right 2 left
- mean age at diagnosis – 76.1
- mean age at onset – 63.3
- pain level – 8-10/10
- duration 3.6 seconds
- stabbing by 5; electric by 3; burning and electric by 1
- tearing and runny nose common in those whose pain shot over eye
- all had touch sensitivity – a finding suggesting botox might be useful- and indeed was, in the one case they used it.
- Aggravating – chewing (5/8), speaking(3/8), coughing (1/8), extreme temperatures (1/8), strong wind (1/8), orofacial movements (1/8).
- 1/2 had pain subsequent to attack lasting minutes to hours but most were not severe
- all had compression of superior cerebral artery on MRI
Treatments:
- 7/8 did well on meds
- 3 did well on one drug: – pregabalin(1), gabapentin (1), eslicarbazepine(1) but these cases eventually had recurrence
- 4 required combination treatment which could include pregabalin, gabapentin, eslicarbazepine, lamotrigine, lacosamide, carbamazepine and oxcarbazepine).
- One of the patients obtained additional benefit from the injection of onabotulinumtoxinA 35 U around the stemming area.
The new treatment was eslicarbazepine (Aptiom):
Cuadrado, María‐Luz, Ángel Aledo‐Serrano, and Lara Ruiz‐Álvarez.
Eslicarbazepine acetate for a patient with highly resistant epicrania fugax.
Pain Practice 15.1 (2015): E27-E27.
no abstract
“Eslicarbazepine acetate is a new anti-epileptic from the same chemical family as carbamazepine and oxcarbazepine. This pro-drug is rapidly converted to active metabolites that stabilize the inactivated state of voltage-gated sodium channels, preventing their return to the activated state and thereby sustaining repetitive neuronal firing. Based on its similarities with carbamazepine and oxcarbazepine, eslicarbazepine is currently being assessed for the treatment of neuropathic pain, including diabetic neuropathic pain and postherpetic neuralgia. One case report in the literature stated that eslicarbazepine was an effective alternative to carbamazepine in trigeminal neuralgia. Likewise, eslicarbazepine might be useful for other headache disorders responsive to anti-epileptic drugs.”
One case epicrania fugax responded to carbamazepine 200 mg qid but made subject too drowsy but was controlled on Eslicarbazepine acetate initially 800 mg/day and titrated to 1600 mg/day.
Comments –
- Another flavour of Trigeminal Neuralgia.
- A previous article on trigeminal neuralgia, http://painmuse.org/?p=156
reviewed neurosurgeon Dr. Anthony Kaufman from Winnipeg perspective on treatment – He suggests starting with microvascular decompression and, if it reoccurs, it is usually easier to treat with pills.
- Eslicarbazepine acetate looks exciting and was required in one case of Facial epicrania fugax – but is expensive and not covered by our drug plan for such indications.
- Botox injections could be a way to treat elderly cases not amenable to anything else (an indeed most were elderly)). I usually found I had to beat down any residual soreness with subsequent 5% lidocaine injections (might take several for a good take) and together could get up to 12 week respite (also mentioned in above link).
- Hope above commentary helped describe some cases not well delineated before.