
A Water pill, Spironolactone 100-200 mg/day, can dramatically relieve pain in potentially 1/2 of Fibromyalgia cases and reduce morphine needs. -NOT CONFIRMED
https://onlinelibrary.wiley.com/doi/pdf/10.1002/ejp.1784
http://www.scandinavianjournalpain.com/article/S1877-8860(14)00006-8/abstract
-
31 cases severe resistant Fm with pain levels 8.8±1.6 /10
- Spironolactone 100-200 mg/day
- within 5 week, and persisted at one year followup, pain dropped to 2.6±1.9 (mean ± SD).
- Mood issues dropped from 35.4/60 to 10.0/60 as did quality of life improve.
- Opioid requirements significantly dropped
- 5/31 noted dry skin; one developed high potssium at 6 months ( I tell people to cut down on oranges and banana to prevent that)
How might it work?
- Has hormonal effect that might help
- Effect GABA receptors and could reduce the sympathetic overload seen in FM cases and help sleep and mood.
- Low dopamine is seen in FM and is associated with restless legs – Spironolactone may effect GABA -dopamine circuits and help the pain
- minerocorticoids promote cytokine inflammation
- Minerocorticoid activation increases excitability of satellite glial cell that can be atenuated through minerocorticoid blockade
- Dong F, Xie W, Strong JA, Zhang JM.
Mineralocorticoid receptor blocker eplerenone reduces pain behaviors in vivo and decreases excitability in small- diameter sensory neurons from local inflamed dorsal root ganglia in vitro.
Anesthesiology 2012;117:1102–12.
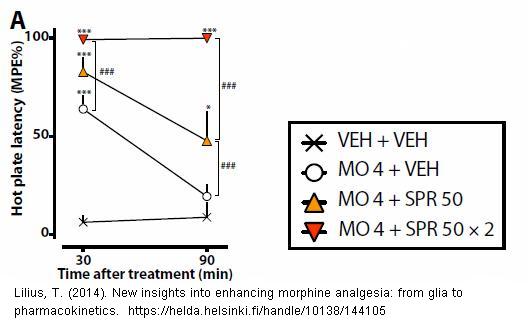
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3482280/ - In the animal model, spironolactone helps morphine work better (opioid sparing). Below animals were given morphine and spironolactone and had nil tail flict responses to pain at hgh dose.
- Minerocorticoid blockade (which spironolactone does) attenuates diabetic neuropathy in the rat model:
Takata, H., Takeda, Y., Zhu, A., Cheng, Y., Yoneda, T., Demura, M., … & Yamagishi, M. (2012). Protective effects of mineralocorticoid receptor blockade against neuropathy in experimental diabetic rats. Diabetes, Obesity and Metabolism, 14(2), 155-162.
http://www.ncbi.nlm.nih.gov/pubmed/21951301 -
This has lead to an hypothesis that diabetic neuropathy is driven by minerocorticoids:
Pro-nociceptive role of the activation of mineralocorticoid receptor in the pathogenesis of painful diabetic neuropathy.
Fei Dong et al.
Medical Hypotheses 81 (2013) 436–438
http://www.sciencedirect.com/science/article/pii/S0306987713002818
An editorial in the same issue:
From patient observation to potential new therapies—Is old spironolactone a new analgesic?
Eija Kalso
- Makes point that pregabalin (Lyrica) and duloxetine (Cymbalta) only significantly (>50%) help 2/10 cases.
- remarkable average improvement
Comment – there realy are no citations to confirm study but results look good. I had one patient with Polycystic Ovaries and diabetes that I thought would be a good candidate. She unfortunately has some inflammatory features (morning stiffness, response to celebrex). She said she had taken Aldactone in the past and noted it helped the skin tenderness pain but seemed to make the joint pains worse… This confirms in my mind that it works more for the small fiber neuropathy sort of pain – not inflammatory. This is an exciting new addition to treatments.
addendum – a foreign language animal study found “spironolactone
caused a fourfold increase in the morphine response” so might be more useful in combination with opioids?
Lilius, Tuomas. “UUSIA NÄKEMYKSIÄ OPIOIDITOLERANSSIN HOITOON. [New views of treating opioid dependence]” Anesthesiology 111 (2009): 1356-64
another of his rodent reports states ” This effect was mediated via the increased access of morphine to the central nervous system by the inhibition of the efflux protein P-glycoprotein. Spironolactone did not inhibit the metabolism of morphine to the pronociceptive metabolite morphine-3-glucuronide, and it did not prevent the development of opioid tolerance.”
Lilius, Tuomas. “New insights into enhancing morphine analgesia: from glia to pharmacokinetics.” (2014).
https://helda.helsinki.fi/bitstream/handle/10138/144105/Thesis-Lilius.pdf
Pingback: Reaching “Critical Mass” to Achieving Pain Control – Procedure Pearls | Pain Medical Musing
Pingback: Mulople Sclerosis (MS) Pain Treatment Options | Pain Medical Musing