
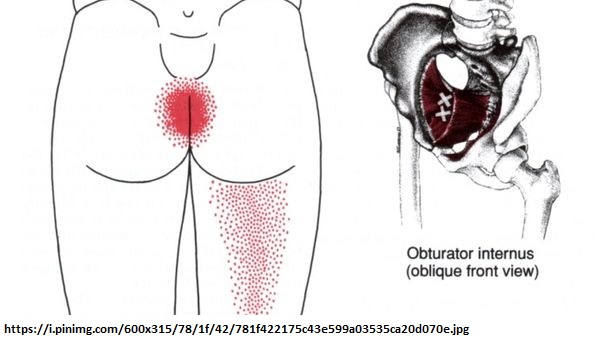
I have a case of long term piriformis syndrome that I have been whittling away for some time. To be fair, she has seen multiple specialists and is some better but not enough to improve quality of life, (old sad joke – If you fix 3/4 problems in chronic pain patient how much better do they feel – answer – not at all – because remaining issue can take them to ceiling re pain) . I found a potential answer in a 2010 thesis from Norway that describes exploration surgery on resistant buttock pain – sciatica cases that found a very contractured obturator internus muscle – a muscle felt pelvically only by palpating the front of the pelvis.
![]()
(I love the image but it looks copyrighted so I only link to image site which is https://www.kenhub.com/en/atlas/musculus-obturatorius-internus)
Meknas, M. Khaled.
Retro-trochanteric sciatica-like pain.
PhD Thesis University of Tromsø, Norway (2010).
https://www.orthopaedics.gu.se/digitalAssets/1312/1312006_meknas-avhandling.pdf
Case I have has pain localized to sacrum and perhaps radiating down leg yet coccyx appears fine.
 Thesis refers to study:
Thesis refers to study:
Windisch G, Braun EM, Anderhuber F
Piriformis muscle: clinical anatomy and consideration of the piriformis syndrome.
Surg Radiol Anat 29:37–45, 2007
doi:10.1007/s00276-006-0169-x
https://link.springer.com/article/10.1007/s00276-006-0169-x
“48 of 112 cadaveric specimens had a fusion of the piriformis and the internal obturator muscles” suggesting if one is in trouble, other will follow
- One of thesis studies involved “Twelve patients, three males and nine females, mean age47 (25–66) years with retro-trochanteric pain in the buttock, radiating distal to the knee and intolerance to sit more than 40 min.
- mean duration symptoms 7.5 years.
signs:
- Positive straight leg raise 10/12 cases
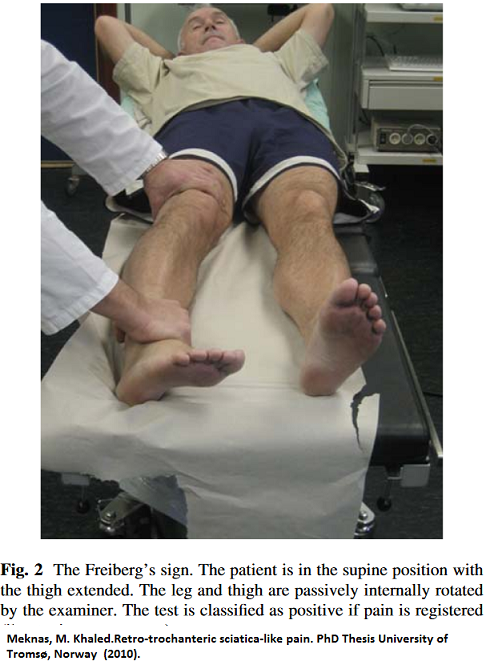
- Freiberg’ sign positive 8/12 moving hip back and forth and seeing if it elicits pain
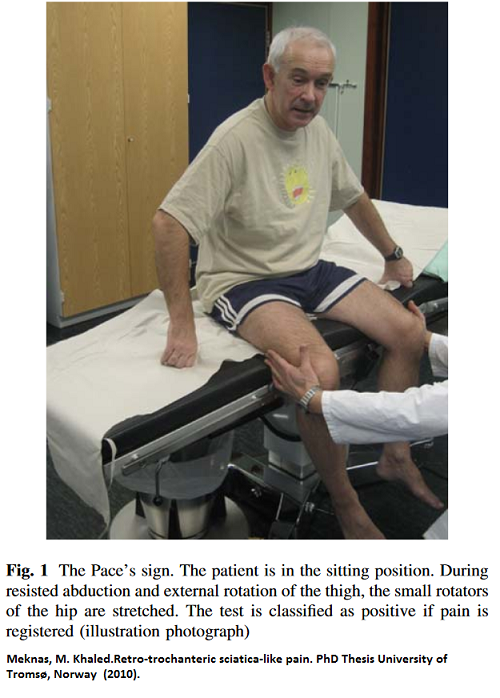
- Pace’s sign positive 10/12 – seated – push knees apart(abduction); hip turn heels in and resist tuning them out (resisted external rotation)
- tenderness on palpation – all
- walking problems – all
randomized half to surgery:
surgical findings:
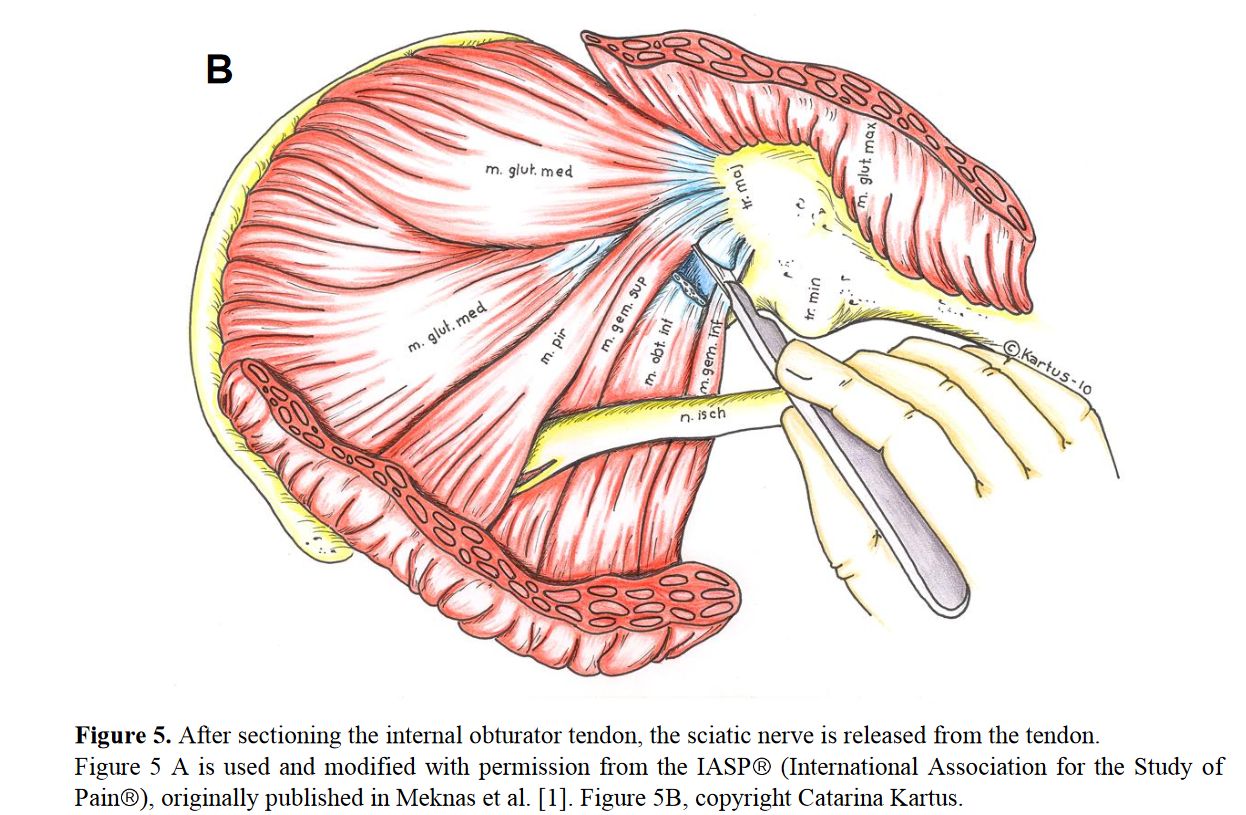
- “The internal obturator muscle was found tense, hyperaemic and in close contact with the sciatic nerve .
- The nerve was flattened and slightly hyperaemic.
- “When performing the Lasegue manoeuvre onthe operating table, the internal obturator, and not the piriformis muscle, impinged on the sciatic nerve at an early stage during hip flexion. To relieve the tension towards the sciatic nerve from the internal obturator muscle, sectioning of the tendon was performed at its insertion to the greater trochanter. An immediate release of the tension towards the scatic nerve during the Lasegue’s manoeuvre [ straight leg raise] was observed after sectioning of the tendon.”
 Results:
Results:
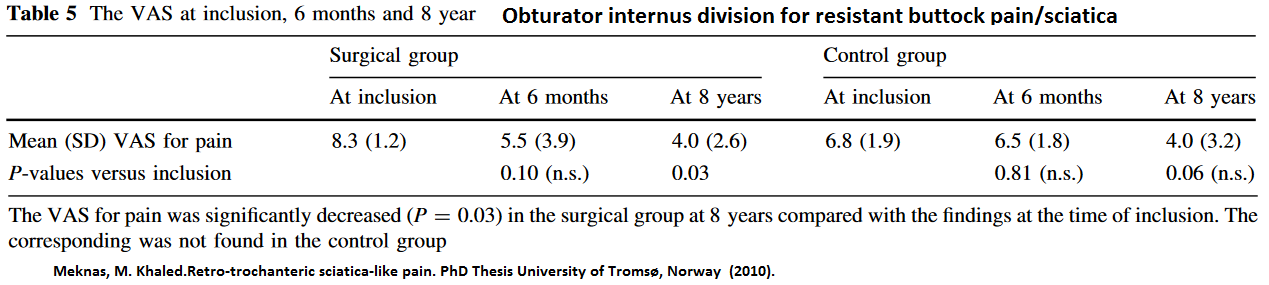
- What is obvious, is the surgical group was definitely worse and reduced pain from an intolerable level potentially managed level with meds.
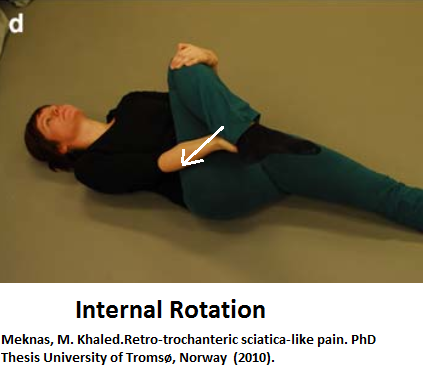
Alternative treatment:
stretches – hold for 15–30 s and repeated 5–15 times; not clear how often were done.



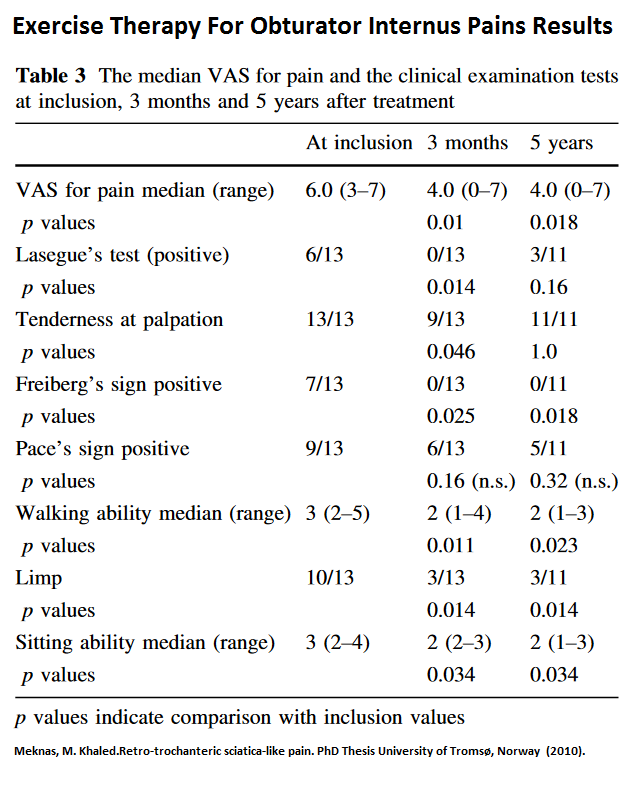 A drop of 2 is a real difference but it is clear these people were not as severe as the surgical group.
A drop of 2 is a real difference but it is clear these people were not as severe as the surgical group.
Comment – a clear reason why piriformis cases might not respond to just piriformis treatment. Can’t wait to check patients for it. The obturator internus forms the front wall of the pelvis – am not sure how sore it will be there.