
Someone wrote:
“I came across this while searching the web. I have bilaterial shoulder impingement, tendonosis, tendonitis, etc etc so they say. I have been in pain since 2002. I have had 2 MRI’s that show nothing. The surgeon says there is nothing wrong but a little arthritis. I cannot sleep at night because if I roll on either shoulder it hurts and I wake up. Sometimes the pain is so bad I go for days without sleeping. It feels as if my shoulders are pulling out of the sockets. I have stabbing pains that sometimes go to the elbows. The surgeon only suggests more physical therapy or more injections….neither of which have done any good. I take pain pills constantly that I am sick of taking because at this point in time they only take the edge off and I refuse to take anything stronger. I am extremely frustrated and don’t know what to do. There IS something wrong…I can’t imagine having to live like this the rest of my life. I was a massage therapist for 10 years and injured them doing 12 massages a day. I keep telling the surgeon that just because he can’t see something doesn’t mean it doesn’t exist. Any suggestions? I’m desperate.”
I generally have great difficulty answering calls for help because it assumes I know what the problem is. There are so many possibilities that this could represent:
NECK CONNECTION
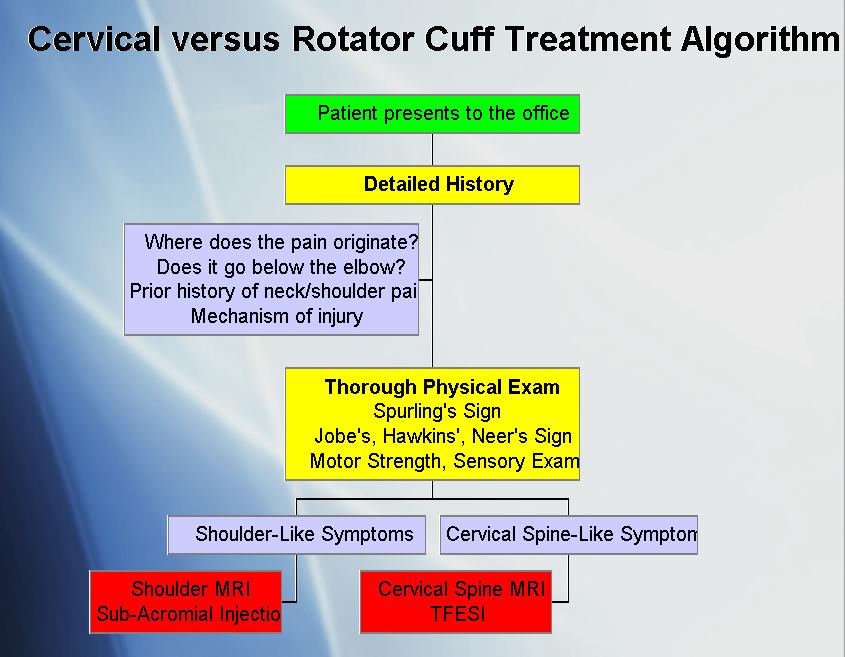
Dr. Kern Singh has written a beautiful power point presentation on the concerns of differentiating neck from shoulder pathology in chronic shoulder problems. It is called:
Differentiating Shoulder Versus Cervical Spin Pathology: A Pain In the Neck
and is available here
He documents his approach such:
I have attempted my differentiation of the two here:
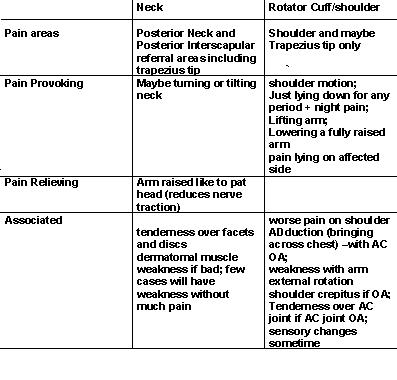 With neck disc disease causing a problem there would also be tenderness in the neck at the incriminating disc level that would not go away with measures to relax the muscle in the area. I have discussed that here
With neck disc disease causing a problem there would also be tenderness in the neck at the incriminating disc level that would not go away with measures to relax the muscle in the area. I have discussed that here
(scroll down in referred site)
I have some obvious questions:
Is there any neck stiffness? Is there pain at end of rotation or sidebending of the neck? The fact the pain can shoot down to the elbow suggests some nerve involvement – does neck movement bring this on occasionally? Often there are a variety of muslces affected with neck problems:
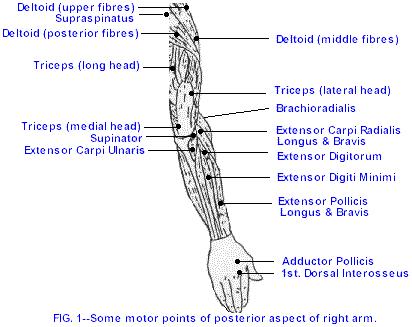
Dr. Chan Gunn found the following muscle activations:
Tennis Elbow and the Cervical Spine article here
(results are % of cases)
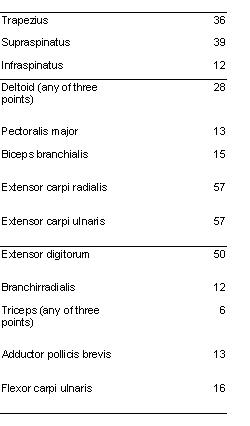
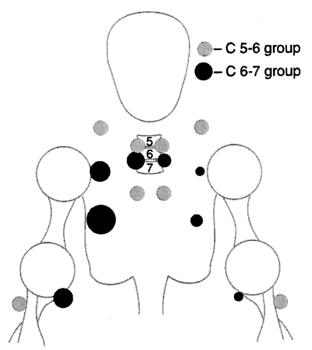
Cervical disc lesions were found associated with certain muscles
J Formos Med Assoc. 1998 Mar;97(3):174-80.
Association of active myofascial trigger points and cervical disc lesions.
Hsueh TC, Yu S, Kuan TS, Hong CZ abstract here
C3-4 lesions with levator scapulae and latissimus dorsi trigger points
C4-5 lesions with splenius capitis, levator scapulae, and rhomboid minor trigger points
C5-6 lesions with splenius capitis, deltoid, levator scapulae, rhomboid minor, and latissimus dorsi trigger points
C6-7 lesions with latissimus dorsi and rhomboid minor trigger points.
Recently the trapezius shoulder tip was shown to be related to the C5/6 facet and injecting that facet deactivated the trapezius tip pains for a period of time:
Injection in the Cervical Facet Joint for Shoulder Pain With Myofascial Trigger Points in the Upper Trapezius Muscle
By Chien-Tsung Tsai, MD, MSc; Lin-Fen Hsieh, MD; Ta-Shen Kuan, MD, MS; Mu-Jung Kao, MD; Chang-Zern Hong, MD; ORTHOPEDICS 2009; 32:557 abstract here
Smythe found a group of fibromyaglia cases which were actual subclinical neck radiculitis (sciatica):
I discussed this under – Upper body “Fibromyaglia” Misdiagnosis here
RIB CONNECTION
To complicate things further, I have found a group that points to their “shoulder” pain as being in the trapezius tip and upper interscapular area. This appears to be more scalene spasm associated with rib positional neuritis that responds some to injections and mobilizations.
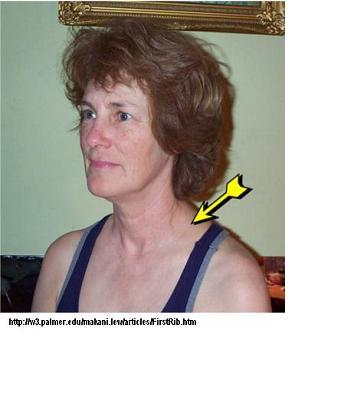
This is discussed by (and pic taken from):
The Elusive (and Painful) First Rib By Dr. Makani Lew, DC
MUSCLE INVOLVEMENT
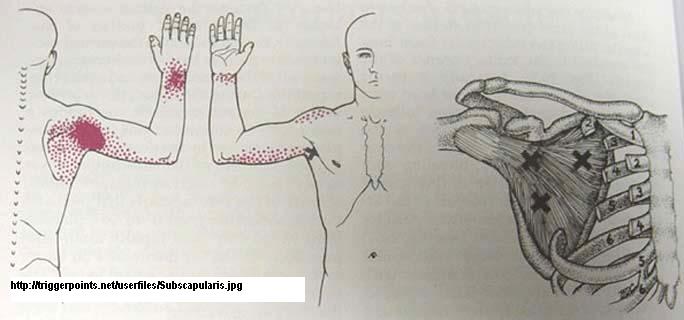
The shoulder muscles play a consistent roll in shoulder problems and I have found the worst to be:
deltoid – anterior, mid and posterior each have unique problems and can be intense. I have had to resort to semi-neurolytic injections of 5% lidocaine into some areas to get anywhere with some of it.
Subscapularis – always bad. Had trouble sleeping on my side and dug my thumb under the scapula in the armpit and massaged it with benefit. NOTE – I have never been able to take out a subscapularis muslce in under 120 rubs – often longstanding 150+ rubs – anybody doing ten or 20 rubs is just kidding themselves.
Now the plot is just beginning to thicken. I had one gentleman who had potentially four issues complicating his case:
1) Neck showed foraminal stenosis (nerves entraped where they come out the sides in the neck) on the side the shoulder was in trouble – I suspect it tightened up the muslces about the shoulder and made the rotator cuff inpingment happen – part of what is called the neck- shoulder syndrome
2) Longstanding widespread pain, 1 hour+ morning stiffness, excellent though temporary, response to cortisone, and a positive HLA B27 test – making the prospects of ankylosing spondylitis a real prospect. The presence of low back pain and stiffness would certainly make this something to be looked into…
3) Typical rotator cuff impingment – catches with arm at shoulder level, trouble with sleep, temporary response to steroid injections – has since had shoulder surgery to deal with impingment and is getting better – and the neck has even settled some too!
4) Depression – always makes the pain worse – Cymbalta helped both the depression and some of the pain though Venlafaxine might work to…
Prolotherapy is an up and coming possibility for the resistant shoulder and I discuss that and other possible treatments under
Resistant Shoulder Tendonitis Treatments here
I am sure there will be other factors that need attention and any comments would be appreciated (come- on you lurkers….)
PS to patient – if this is rotator cuff disease, you will sleep much better sitting up in a recliner chair where gravity will traction the shoulder joint down some and relieve pressure on the rotator cuff. If this is more just muscles, then perhaps a memory foam overlay might help (helped me)… If this is neck related, then a cervical traction device would make a difference… Neck Cheap Cervical Traction here
Addendum:
Patient has since added:
“If I were a pro-football player or pro-rodeo rider I believe the doctors would have taken me more seriously. I know at least two people that had a scope when nothing showed up on the MRI and with the scope they found tears of the rotator both times. This effects everything I do. It hurts to raise my arms, putting my arms behind my back is almost impossible, just my arms hanging at my sides gives me the feeling of them pulling out of the sockets. I do have stenosis at C 3 or 5 and slight arthritis, but had that before the shoulder pain. I just got a memory foam 4 inch for my bed and it is wonderful but does nothing for the shoulder pain. I also have a cervical traction device that I will try using more. I also use a tens unit that works for the moment. The pain shooting down to the elbow subsided after the first year except on occasion. The pain is most of the time like a toothache that never goes away but sometimes it is like a stabbing pain. I’m just at a loss, but I do know one thing….I’m not crazy, there is something wrong.”Now it is getting even more complex with at least 4 issues surfacing:
1) Certainly C5 foraminal stenosis would refer to shoulder. A selective nerve block of C5 would help delineate that; but given there is a radicular spinal artery that comes out at C5, and this vessel can be inadvertantly threaded by injection, that could be a risky business. Having said this,
Skeletal Radiol. 2007 May;36(5):431-6. Epub 2007 Mar 6.
Cervical interlaminar epidural steroid injection for neck pain and cervical radiculopathy: effect and prognostic factors.
Kwon JW, Lee JW, Kim SH, Choi JY, Yeom JS, Kim HJ, Kwack KS, Moon SG, Jun WS, Kang HS
abstract here
“Cervical radiculopathy consisted of shoulder pain, arm pain, or both”
They injected the nerve root at a particular level with freezing and cortisone.
their cases included:
Neck pain only – 13 cases – 69% responding to injection
shoulder/arm pain “radiculopathy” – 33 cases; 79% responding to injection
neck/shoulder arm pains = both neck and radiculopathy 30 cases – 67% responding to injection.
In our city, Dr. Mike Lang, a pain specialist and anesthetist, prefers to do steroid epidurals done at C7 the traditional way and gets results. The gentleman I I treated above (with foraminal stenoisis) had a cervical steroid epidural but it only gave temporary relief.
2) Shoulder pain, worse at night, and with worsening on raising (?painful arc) – initially shoulds like a shoulder tendonitis or more likely, a shoulder subdeltoid bursitis. Sounds like patient had had steroid injections into area which were only temporarily beneficial. Calcifications in the tendons offer a possilbe site of treatment discussed here
3) Persistent shoulder pain with some restricted movement – sure sounds like a shoulder capsulitis – a “frozen shoulder” – a one joint autoimmune disorder that scars up the joint and leaves the joint painful especially at night for 1.5 years+ before loosening up. When the pain gets bad, the pain can go down arm. Treatments include
- arthritis pills
- home exercises,
- (?repeated) shoulder steroid injections,
- shoulder capsule stretching by “hydaulic distention”, abstract here
- manipulations,
- physiotherapy,
- muscle work (injections, needling, massage, stretching),
- regional suprascapular nerve injections,
- time.
4) A persistently inflamed shoulder – I recently had an older lady with bilateral shoulder pains that had seen an orthopedic surgeon and had both shoulders injected with steroid with temporary benefit. he told her there was nothing else he could do. She also complained of weight loss and widespread pain. I thought she could be a polymyaglia rheumatica as they can present with shoulder pain and worried she might have an occult malignancy with it.
polymyalgia rheumatica discussed here
Malignancy workup which included chest Xray, abdominal US, CEA, OB stools, etc was all negative. She did have an elevated ESR and CRP and a high anti – CCP
anti-CCP discussed here as a test for Rheumatoid arthritis
She also had a high rheumatoid factor.
She was seen by a rheumatologist who diagnosed her with rheumatoid arthritis and started her on, among other things, methotrexate. I suspect she is going to feel much better.
5) Neck shoulder syndrome – neck problems will tighten up the shoulder and shoulder problems will tighten up the neck. I hate it. The combination makes it difficult to get any sustained benefit. The one recent case I had didn’t get better until he had surgery. The same has been seen with lumbar spinal stenosis and hip arthritis – treat one or the other surgically, and the other problem will settle some.
What does this mean for current patient?
1) Get a full workup –
CBC blood count
ESR and CRP as tests for inflammation
connective tissue disease tests”
RA factor and anti-CCP for rheumatoid arthritis
ANA (for lupus like conditions) – not as useful unless you have rash, hair loss etc.
I run routine rests of thyroid function, testosterone function in men and women, serum B12 and vitamin D levels, and so on in chronic pain patients.
Other tests that depend on history of Tick bites, infection illness prior to problems, etc.
full physical
2) Have a small amount of local injected into shoulder – does that remove a significant amount of pain? It won’t take out all as there will be significant muscle problems. It would however, suggest a frozen shoulder and there are specific treatments for such.
3) If there is significant neck issue and cervical traction helps a bit then consider a cervical epidural at a pain clinic. Alternatively, a shot of etanercept can be given into the muscle on the side or in between the spinous processes. I think this could become a new test for diagnosing radiculopathy. I discuss it here
4) Get the neck and muscles worked on. One approach is called Intramuscular stimulation was developed by Dr. C. Gunn
site here:
They have a list of possible therapists.
5) If neck is clearly a problem, consider getting neck disc therapy.
walk one’s fingers up a wall is another
If I were a pro-football player or pro-rodeo rider I believe the doctors would have taken me more seriously. I know at least two people that had a scope when nothing showed up on the MRI and with the scope they found tears of the rotator both times. This effects everything I do. It hurts to raise my arms, putting my arms behind my back is almost impossible, just my arms hanging at my sides gives me the feeling of them pulling out of the sockets. I do have stenosis at C 3 or 5 and slight arthritis, but had that before the shoulder pain. I just got a memory foam 4 inch for my bed and it is wonderful but does nothing for the shoulder pain. I also have a cervical traction device that I will try using more. I also use a tens unit that works for the moment. The pain shooting down to the elbow subsided after the first year except on occasion. The pain is most of the time like a toothache that never goes away but sometimes it is like a stabbing pain. I’m just at a loss, but I do know one thing….I’m not crazy, there is something wrong.
Wonderful goods from you, man. I have understand your stuff previous to and you’re just too excellent. I actually like what you have acquired here, really like what you’re saying and the way in which you say it. You make it enjoyable and you still take care of to keep it smart. I can’t wait to read far more from you. This is actually a terrific site.