
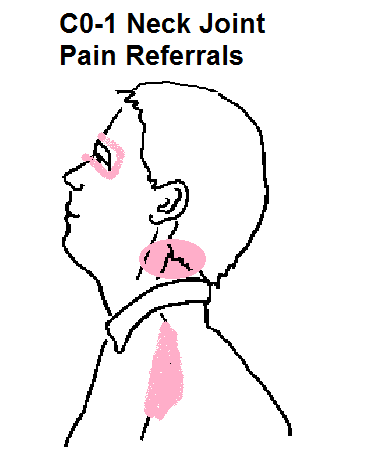
Top joint C0-1 refers to upper neck, face and upper shoulder tips. Exam requires you to grip c1 transverse processes and nod neck sideways. Certain manual techniques might help.
Lee, Dong-Gyu, et al.
Effectiveness of intra-articular steroid injection for atlanto-occipital joint pain.
Pain Medicine 16.6 (2015): 1077-1082.
https://academic.oup.com/painmedicine/article/16/6/1077/2460567?login=false
- 20 cases
- Pain was suboccipital, periorbital, suprascapular, and sometimes temple & forehead. 70% had cervicogenic headache complaints.
- Pain level average 5.6/10
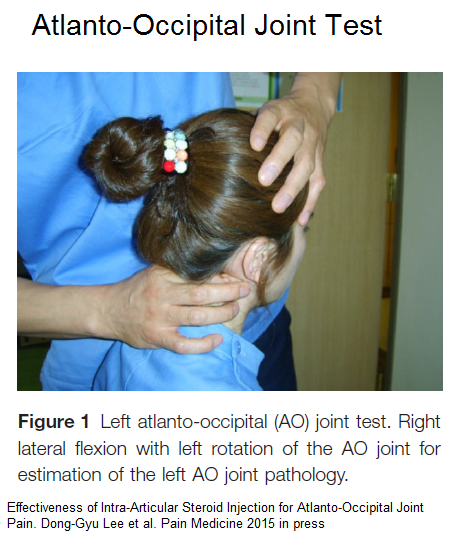
- Exam involved grasping the C1 transverse processes, turn head some to side going to test, and nodding head sideways away from side testing: C1 transverse is felt just behind the jaws.
- this should reproduce pains or be restricted
- Verbatim injection technique:
“The patient was placed in a prone by placing a towel or blanket under the chest to ensure sufficient flexion position of the cervical spine to avoid needlecontact with the occipital brim. The C-arm was positionedwith cephalic tilting to visualize the AO joint, and then theC-arm was rotated ipsilaterally approximately 30°. A 25-gauge, 3.5-inch spinal needle was carefully guided directly through the soft tissue in the upper-most portion of the AO joint. If the needle tip contacted theperiosteum around the AO joint, the C-arm was rotated contralaterally by approximately 30° to show that the needle tip had penetrated into the AO joint . Once joint entry was accomplished, a small amount(<0.3 mL) of radio-opaque contrast media was injected toconfirm the needle position and joint capsule pattern in thelateral view . Next, 1 cc of 2% lidocaine or amixture of local anesthetic (2% lidocaine, 0.75 cc) and steroid (triamcinolone 10 mg, 0.25 cc) were slowly injected for diagnostic block and therapeutic injection,respectively.”
- Results –
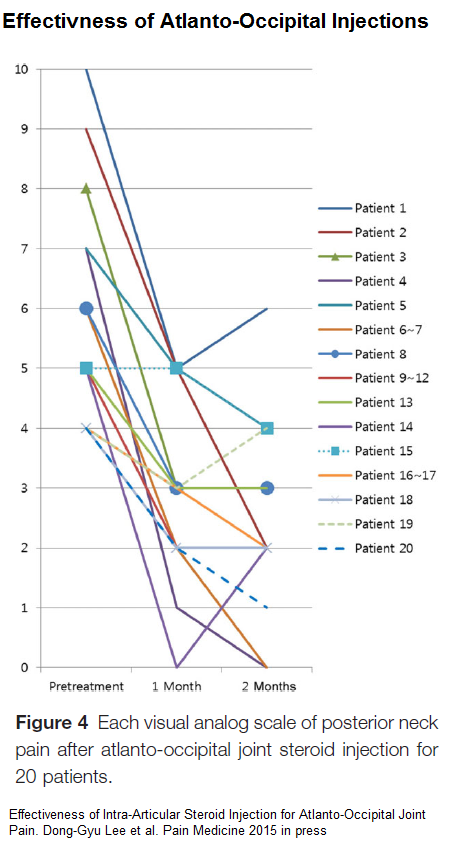
- No side effects recorded
Comment – They could only find 2 cases prior injection result reports so I haven’t found anyone local to do it.
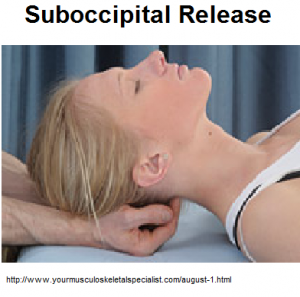
Manual techniques include:
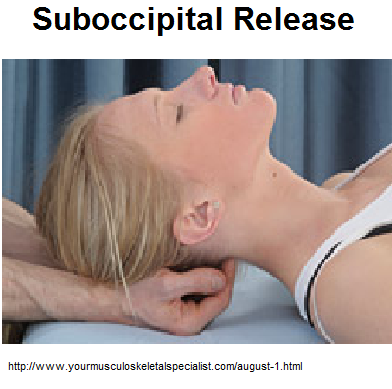
- Suboccipital release: -put bend fingers near midline suboccipitally and just hold fingers there or stretch neck down some – patients love that one – if you are in contact with a tender spot – just move fingers out a bit . – How long? never very sure.
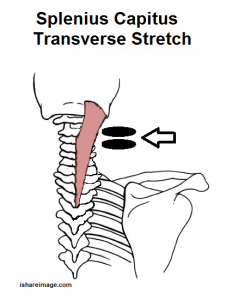
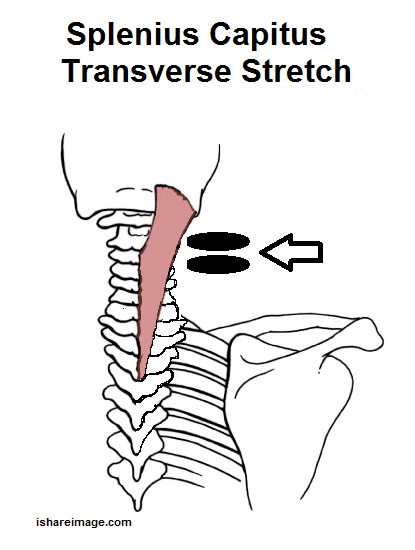
- Suboccipital transverse stretching -the splenius capitus is often very tight and engaging it laterally or medially and then dragging it across can stretch it:
- Suboccipital strip – put finger suboccipitally medial or lateral and strip across- working out tight bands as go – can be very painful as is above – burns
- Suboccipital shake – pinch muscle medial and lateral suboccipital and shake 120 times to see if will loosen up
- Lewitt suboccipital stretch – put thumbs on lower edge of eyeball sockets and hands behind head. Look up for 15 seconds to confuse muscles then rotate head down as you look down (this is not a neck flexion- it is a head rotation) – repeat 3 times
- Mulligan suboccipital stretch: put fist between chin and chest and flex head over it with the help of your other hand
- C1 transverse process work – if you grab C1 transverse behind mid jaw and shake it, it should move slightly. If stiff, loosening up sometimes helps. Some Chiropractors have an instrument you can thump the transverse process – even shown doing so reduces Blood pressure:
J Hum Hypertens. 2007 May;21(5):347-52.
Atlas vertebra realignment and achievement of arterial pressure goal in
hypertensive patients: a pilot study.
Bakris G(1), Dickholtz M Sr, Meyer PM, Kravitz G, Avery E, Miller M, Brown J,
Woodfield C, Bell B.
http://www.ncbi.nlm.nih.gov/pubmed/17252032
I have found nodding head forward by transverse pressure over vertex with palm of your hand and pushing on either transverse process simultaneously can loosen it up. - Rocobano style suboccipital mobilizations:
– lie on back with chin up some
– tilt and turn head very slightly to one side
– push against hand gently to try and straighten from turn/sidebend
– put up chin more slightly, rotate very slightly ( never more that 10-15 degrees) and repeat twice with progressive movement each time
– repeat with head turned and sidebent other direction
People with suboccipital headaches are amazed how much relief can be obtained that way. Can’t claim it works for active Osteoarthritis of C0-1 though.