
A sustained 40% improvement was obtained from direct current 1.5 milliamp voltage – about what a 9 volt battery hooked up with a 10 k potentiometer resistor could furnish.
J Pain. 2015 Apr 8. pii: S1526-5900(15)00606-9. doi: 10.1016/j.jpain.2015.03.013.[Epub ahead of print]
Immediate and sustained effects of 5-day transcranial direct current stimulation of the motor cortex in phantom limb pain.
Bolognini N(1), Spandri V(2), Ferraro F(3), Salmaggi A(4), Molinari AC(5), Fregni F(6), Maravita A(7).
http://www.ncbi.nlm.nih.gov/pubmed/25863170
Direct Current Transcranial Stimulation (tDCS) is not pulse therapy it is simple direct current running from positive anode in this case, near midline, to controlateral negative cathode on lower forehead above eye.
- 8 cases – cross-over, double-blind, sham-controlled design
- pair of surface saline-soaked sponge electrodes.
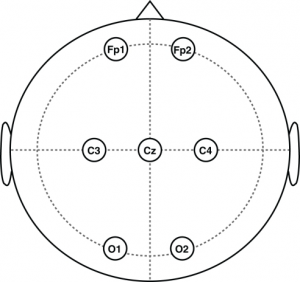
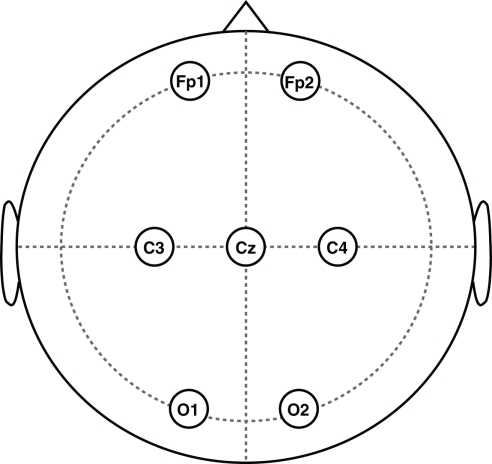
- “anodal electrode was placed over C3 or C4 (EEG 10/20 system) in order to stimulate M1 contralateral to the amputation, while the cathode electrode over the contralateral supraorbital area.” C3/4 is at ear level near midline for leg
- 30 minutes tDCS 1.5 milliamps for 15 min quickly ramped up and down at ends
- “The electrodes (35 cm X 2) were firmly attached by elastic bands, and an electro-conductive gel”. Using pi R square gives me a radius of 3.3 cm or diameter of 6.7 cm.
- 5 days of treatment
Some bits of wisdom:
- “massive sensorimotor cortical reorganization occurs in the cerebral hemisphere contralateral to the amputation”
- “in order to produce analgesic effects, brain stimulation should be applied to the motor cortex contralateral to the side of pain “
- ” in the treatment of chronic pain, motor cortex stimulation with rTMS may be more effective when the stimulation site is adjacent to the cortical representation of the painful zone, rather than within the painful zone itself.”
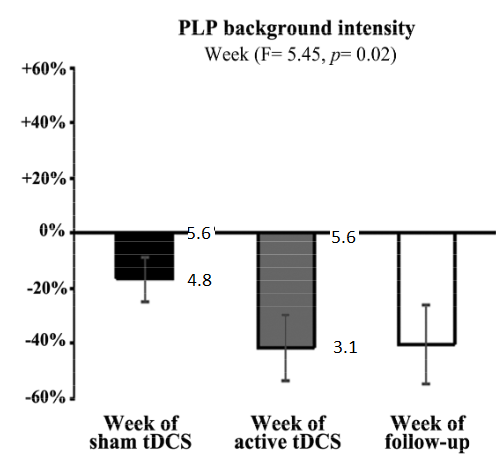
RESULTS: – intensity of pain dropped from 5.6 to 3.1. Frequency of spasms dropped 40% as well. These benefit persisted….
Comment –
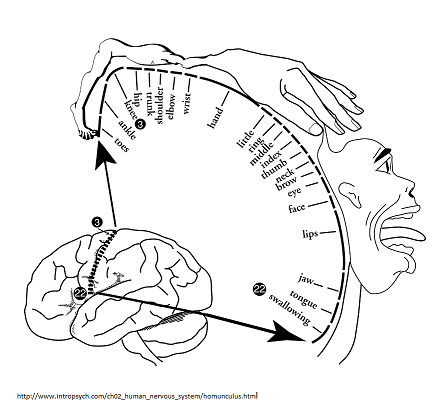
well according to homunculus, the leg would be near the midline:
For the contralateral supraorbital cathode, an ECG pad should suffice: – clean area with alcohol first.

I rigged up a welders head gear to hold the saline pad (hint- put soap in electrolyte- conducts much better).

A 9 volt battery connected to a 10 K potentiometer would be all you would need for electronics. They used to use 2 ma and that was some robust sensation so suspect 1.5 ma is a milder sensation – just turn it up until nicely tolerable.
Good luck with that.