

About 30 years ago, I attended a course given by Drs. Travell and Simon. Dr. Simon was discussing interscapular pains and Dr. Travell mentioned – don’t forget the scalenes – something that Dr. Simon replied he was getting to – as a cause of unilateral interscapular pains. Now, discussion of Dorsal Scapular Nerve entrapment as a cause of interscapular pains has returned, and has helped to highlight a couple cases I am having trouble with. Have you got rhomboid triggers that won’t settle? – Better think of this.
(note also a good article to read is: Dorsal Scapular Nerve Syndrome by Hans Boehnke, D.C. DIBAK http://balancedstructure.com/files/Dorsal_Scapular_Nerve_Syndrome.pdf )
Arch Phys Med Rehabil. 2013 in press
Role of Dorsal Scapular Nerve Entrapment in Unilateral Interscapular Pain.
Sultan HE, Younis El-Tantawi GA.
http://www.ncbi.nlm.nih.gov/pubmed/23220342
- Found in 55 cases of unilateral scapular pain, 52.7% showed electrophysiologic conduction studies consistent with a dorsal scapular nerve lesion and 16.4% with scapular winging from rhomboid weakness.
- average early 40’s with average duration of 10 months and an average pain intensity of 5.5/10; those with electrodiagnositic positive 6.06/10
———————————-
Unilateral Interscaplar Problems were differentiated into:
- Rhomboid major myofascial pain (21) – taut twitchy bands rhomboid major
- Thoracic strain (11) – “Middorsal paravertebral pain and tightness, spastic tender paravertebral muscles, crackling sensation, painful limited flexion and rotation of the spine, no pain referral, and negative radiological findings”
- Thoracic facet (2) – “Paraspinal midback pain that was referred to the shoulder blade and was not increased by coughing, deep breathing, or sneezing; Localized tenderness of the affected facet joint; Positive spring test; Pain was provoked by 3-dimensional motion; Spondylodegenerative changes on plain radiographs at T4- 6 segments.” I usually see below all transverse processes rotated left so left transverse processes prominent underneath and the level above rotated right associated with temporary relief with manipulation or activator thumping.
- Thoracic disc (2) – “Middorsal intermittent electriclike pain that was radiating to the interscapular region with exacerbation of pain by coughing and sneezing, no weakness or sphincteric disturbance, limited painful thoracic flexion, painful axial rotation, hyposthesia along T5 dermatome (1 patient) and along T6 dermatome (1 patient), and degenerated disk at the T5/6 level with marginal sclerosis and osteophytes.” I would also include rather severe pain not relieved easily by mobilizations.
- costovertebral joint dysfunction (1) – “Deep aching pain felt between the scapula and the spine, referred to the shoulder blade, and exacerbated by deep breathing and coughing. Pain was reproduced by palpating the costovertebral junction with tenderness of the rib angle. Spring testing to the rib was positive. Uniplanar side-bending to the affected side elicited the most severe pain. Unremarkable radiological findings.” I usually find remission of symptoms by massage of intercostal muscles at that level anteriorly.
- levator scapula syndrome (1) – “Upper back pain felt over the upper medial border of the right scapula with aggravation by desk job activities using a computer; – Tenderness was felt over the insertion of the levator scapula on the inner border of the scapula; Contraction of the levator scapula during examination was painful and was associated with crepitation; Pain was elicited by scapular downward rotation and adduction. Negative radiographs.” I find head forward posture an issue. If you curl fingers on transverse processes at cervicothoracic junction – can engage muscle and if you pull muscle tight band back until releases (4-10 minutes) you will find rotation to opposite or same side improves.
- Dorsal scapular entrapment: – (9)
– Pain along the medial border of the scapula (9 patients) with itching sensation (2 of them) and radiation to the shoulder (3 patients)
– Exacerbation of symptoms by neck rotation and extension (4 patients)
– Scapular winging (subtle in 3) that was accentuated by active shoulder flexion and abduction, by overhead placement of the arm, and when the arm was lowered from the elevated position
– Pinprick sensation was diminished in an area just medial to the scapular border (1 patient)
– Rhomboids muscles were wasted with reduced strength
– Hypertrophy of the scalenus medius and tenderness over the lower third of the muscle (4 patients)
– Elongated transverse process of C7 on plain radiographs - none 8
Pain Description: – Pain medial border of scapula may be only complaint and it has been suggested this is greatly underdiagnosed.
unilateral interscapular pain – all; some have characterized it as a dull ache:
Dorsal Scapular Nerve Syndrome
Hans Boehnke, D.C. DIBAK
http://balancedstructure.com/files/Dorsal_Scapular_Nerve_Syndrome.pdf
Summary of findings in all their unilateral interscap cases:
- radiation to ipsilateral shoulder 7; down arm -2
- deep aching – 11
- burning – 15
- knifelike – 3
- 2 itching sensation
- 2 sudden onst after heavy lifting; rest more gradually
- 9 repeatative use – teachers, painters, electricians, volleyball, basketball
Signs:
- Rhomboid triggers
- scapula more laterally located on symptomatic side – 9
Hans Boehnke (ref above) wrote: “I have personally found that if I put my thumbs on the inferior angle of the scapulae bilaterally and have the patient abduct both arms as high as possible, that the inferior angle of the scapula on the affected side will travel farther laterally in the direction of the mid axillary line. This is made more dramatic if the patient puts their cervical spine into extension which would increase the entrapment in a case of a hypertonic medial scalene muscle on the involved side.” – I’ll have to look for that. - rare scalene hypertrophy
- rhomboid wasting and perhaps levator scapula wasting as well
- tenderness lower 1/3 scalene – (4) – can refer to scapular area or down forearm if you massage area to see if will work out.
————————
Course DSN:
-comes from C5 spinal nerve root = most upper branch brachial plexus – being essentially motor, missed as cause interscapular pain
- Starts by entering Interscalene groove/ triangle – between scalene anterior and mid
- This triangle is felt by putting your fingers just behind the sternomastoid and moving fingers up from clavicle – the deep muscle just back of the sternomastoid is the middle scalene:

- The dorsal scapular nerve comes out this space and can immediately penetrate the middle scalene muscle:

- It apparently transverses muscle more posteriorly where muscle is more tendonous:
Dorsal scapular nerve compression── atypical thoracic outlet syndrome.
Cheng Desong,Gu Yudong,et al.
CHINSES JOURNAL OF HAND SURGERY 1994-01
http://en.cnki.com.cn/Article_en/CJFDTOTAL-ZHSK401.013.htm - Courses posteriorly to just under the levator scapula to upper inner angle of scapula.

- Comes more superficial between rhomboid minor and major and courses down by side of scapula under trapezius. Innervates Rhomboid major and minor.
- The accompaning artery feeds the lower end of trapezius.
- At superior angle scapula it is 1 cm medial and 2 – 2.5 cm deep. There is an accompaning artery is about 2.75 mm at upper and 1.75 mm at lower end – perhaps a doppler can find it…
Entrapment;
- Anteriorly, this would be felt at C5 where it enters the mid scalene (felt as muscle in triangle just behind sternomastoid). They thought less than 1/2 of pure DSN sydrome cases were tender there.

- An article was written about C5 entrapped by scalene causing neck pain and unilateral shoulder weakness.
Analysis of 25 cases of neck-shoulder-pain accompanied with weakness of shoulder abduction
Chen Desong, Fang Yousheng, Peng Feng, et al.
Chinese Journal of Hand Surgery 1997-03
http://en.cnki.com.cn/Article_en/CJFDTOTAL-ZHSK199703005.htm
The most distinguishing features were:
“The most obvious tenderness point was located at the juncture of external jugular vein and posterior margin of sternoclaidomastoid muscle. Impairment of sensation was manifested as deereased sting at medial antebrachial area and the ulnar side of the hand.” I’ll have to check that point.
Posteriorly in should be felt at the anterior border of the vertebral body of c5/6;
Three mechansims have been suggested for pain:
- nerve entrapment like thoracic outlet syndrome. Apparently 10% of scalene medius have an actual band in it.
- Secondary triggers in rhomboids (I would suggest in trapezius near T2-3 medially and posterior deltoid as well)
- Muscle triggers causing microentrapments of dorsal scapular and cutaneous thoracic branches with pains. I like to hit these microentraped areas with 5% lidocaine (max 1.5-2.0 mls and stay clear of spine) – takes up to 3 times for good take but can give relief for weeks or longer.
Most Important Finding: “Cases with Myofascial Pain Syndrome [trigger knots] of the rhomboids that are resistant to treatment should be evaluated for possible entrapment of the DSN.”
I have injected botox into this C5 area (without local) and found it helpful for unilateral interscapular pains. Injection local to area by C5 could be dangerous as there are numerous vertebral/cervical and cranial arteries in areas and just because you cannot draw blood back with syringe is no help (only 50% accurate). Injecting onto bone allows you to skewer an artery and local will seep back into it (one death so prolotherapists take note).
I will have to discuss physio etc but not today.
A chinese review of 128 cases found pain point injection into neck and by T3 and T4 spinous process resulted in good recovery after 1 – 6 sessions with results being better if they had symptoms for less than 6 months. They felt people could feel relief within minutes of injections.
Clinical analysis of 128 patients with dorsal scapular nerve compression syndrome treated with pain-point injections
LIU Qingjun, ZHANG Xiaoping, XIA Ping, ZHU Jun, LI Jianmin
Pain Clinic Journal, Year 2010 , Issue 1 , Page 10-12 http://www.cqvip.com/Read/Read.aspx?id=33576998
Curative treatment involves cutting scalene medius and maybe anterior as well. http://www.cqvip.com/Read/Read.aspx?id=33576998
and in:
Dorsal scapular nerve compression── atypical thoracic outlet syndrome.
Cheng Desong,Gu Yudong,et al.
CHINSES JOURNAL OF HAND SURGERY 1994-01
http://en.cnki.com.cn/Article_en/CJFDTOTAL-ZHSK401.013.htm
surgery cured 19/20 cases.
_______________________
Addendum
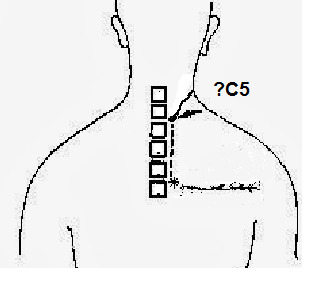
Since I have been injecting tender cutaneous nerves as a treatment I have come across interscapular nerves that are very tender:
1) They course horizontally just below spine of scapula
2) They approach t4 or 5 spinous process
3) It then courses horizontally up to T2 – this vertical nerve will be about 1 cm from spinous process, palpable and tender.
4) an oblique tender line from T2 up to where would expect dorsal scapular nerve to course
5) Lower cervical facets will be obviously tender.
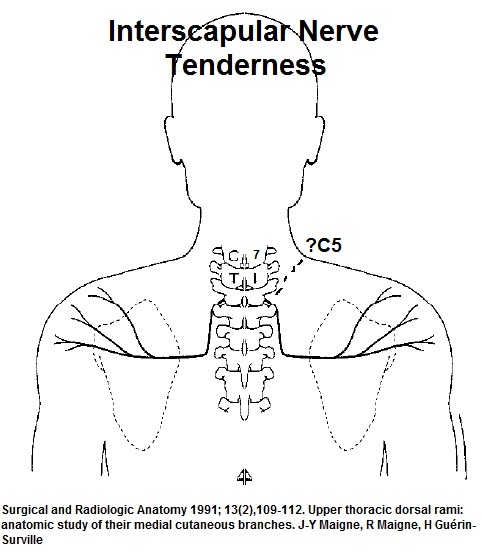
This corresponds to an interthoracic connectioned mentioned in a previous anatomy article:
Surgical and Radiologic Anatomy 1991; 13(2),109-112.
Upper thoracic dorsal rami: anatomic study of their medial cutaneous branches.
J-Y Maigne, R Maigne, H Guérin-Surville
http://link.springer.com/article/10.1007/BF01623882
They found one possible interscapular cutaneous nerves to be:
 I have been injecting D5W with 3% glycerin along both deeper dorsal scapular nerve tract and along this interscapular T2 dorsal nerve root with anomalous course. I inject shoulder tip areas and use an activator to manipulate cervical facets or inject small amounts of botox into facet joint (no local) at about C5 level.
I have been injecting D5W with 3% glycerin along both deeper dorsal scapular nerve tract and along this interscapular T2 dorsal nerve root with anomalous course. I inject shoulder tip areas and use an activator to manipulate cervical facets or inject small amounts of botox into facet joint (no local) at about C5 level.
Addendum:
One differential diagnosis of unilateral scapular pains is Scapulothoracic Bursitis which was recently written up:
Rheumatol Int. 2014 Feb 20. [Epub ahead of print]
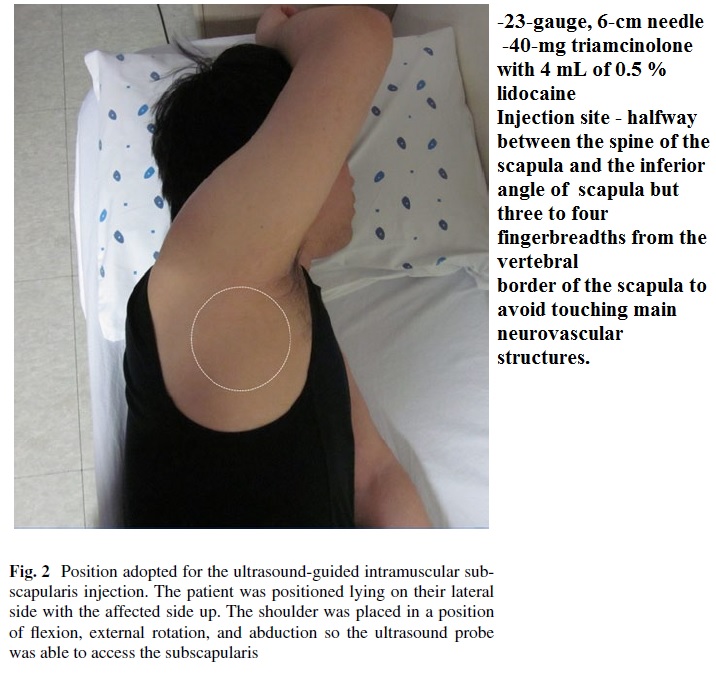
Comparison of the therapeutic effects of intramuscular subscapularis and scapulothoracic bursa injections in patients with scapular pain: a randomized controlled trial.
Chang WH(1), Kim YW, Choi S, Lee SC.
http://www.ncbi.nlm.nih.gov/pubmed/24553678
Some of the criteria used would be:
1) Moderate severity – their cases had an average pain of 7.7 though I saw one today with only a 3/10.
2)”Extreme” pains are right on edge of scapular border – superior angle and mid edge
3) They did accept people with shoulder and neck issues
4) A history of a snapping scapula would be nice though they excluded them in their study for some reason
They preferred a lateral approach with patient’s arm up:
Results of injection
– blind injection pain went from 7.7/10 to 3.5/10
– ultrasound guided went from 7.8/10 – 2.9/10
This is a statistical difference but not clinical. They did mention there was subscapularis muscle pains. In the axilla, I put my thumb or fingers on inner scapular edge and rub 120 times (never got it to release in any less) – the subscapularis muscle will release – might have been worthwhile to see if there was even a statistical difference after that. I inject through a medial approach and hope that neurovascular bundles are anesthetized given a block as well as steroid injection..
I have discussed it here:
http://painmuse.org/?p=944
I have suffrered for six years with this kind if pain, I live in Atlanta , Ga and have yet to find any doctor that has even identified the problem let alone fix it! If anyway knows of a surgeon that is hi this discipline please advise.
————–
People dealing with chronic pain in US might be a member of the American Pain Society:
APS
http://americanpainsociety.org/
I strained my right shoulder 6 mo ago, diagnosed as a Teres minor strain, done PT and had minimal improvement. I now have bilateral or a times alternating inter scapular pain and spasms worse at night. I also live in Atlanta. I think I possibly have one of the syndromes listed above. Is there some one in Atlanta that I can seek for an evaluation?
Hello, I’ve been hit by these symptoms for years… and it seems everything you are talking above corresponds at my situation. What can I do to heal this? I live near Toronto, Toronto. Can you suggest me a specialist who could help me to treat that?
Thanks!
Dominic D.
———
Canadian Association of Orthopaedic Medicine (CAOM) maintains a website here:
http://caom.ca/
You can request help in finding someone in Toronto. Good luck
admin
I find this page fascinating because it perfectly details what has been ailing me. I incurred this injury wrestling in highschool over ten years ago and simply cannot find permanent relief. I have been to several rehabs and chiropractics which have helped, but the treatment doesn’t last. Is this something that I can try to fix with acupuncture, or does it need actual surgery?
Before seeking professional treatment, try working on your deep neck flexors and scapular muscles to relieve the tension on the nerve.
Deep neck flexors – a million on youtube (nodding in supine).
scapular muscles – plank (from knees if req’d) with neck ‘packed’ (Eric Cressey) and shoulder blades down and back. Sounds easy, it’s not.
Try those for a while. Therapy only opens up a window in which to exercise. It’s the exercise that keeps you better.
I am a radiologist working in Europe.
Only after 16 years I managed to figure out what I have which is dorsal scapular nerve entrapment with rhomboid dysfunction-paresis.
First manifestation was a thrombosis of a my subclavian vein ( likely due to a hypertonic middle scalene or anterior scalene) though NO TYPICAL thoracic outlet syndrome symptoms after this.
My pain is mostly medially to scapula with fatigue, burning sensation and a dull sensation affecting all the surrounding muscles that compensate for the nonfunctioning rhomboid.
I have injected botox to my middle scalene with just mediocre results.
Will get a MR neurography soon and will decide after conservative treatment ( or some additional botox) to eventually go and remove my scalene ( or resect a band if they find it).
Very hard to diagnose stuff.
I have had this syndrome for over two years. My main symptom is levator scapulae athrophy on my right side, which led to scapular winging. Any sort o arm movement is affected because my levator scap does not activated. This severely hinder the proper function of my scapula during upper body excercise. I have been to many doctors that and they say it is thoratic outlet syndrome but an emg concluded that my serratus was functioning properly. I beleive my Dorsal Scapular nerve is entraped (probably in mid scalene muscle) In addition to my levator scap, I think that my scalene muscles are also athrophied because there is a veterbrae proccess sticking out (there is no muscle covering it as opposed to the other side of my neck) Is this dorsal scapular nerve entrapment, and if so can anyone direct me to a specialist who can treat this? thanks.