
Diabetic peripheral neuropathy with pain, and numb feet and toes could be the result of an entrapment like carpal tunnel and hence potentially treatable. However considerable controversy follows it.
Diagnosing entrapment of nerves in the leg (Tarsal Tunnel Syndrome) is frought with considerable problems as exemplified by carpal tunnel:
1) Carpal tunnel entrapment is now thought to be a tendonopathy induced disease (one current approach is to actually strip down the swollen tendons as a treatment).
2) Response to carpal tunnel surgery has very little to do with the delineated nerve conduction entrapment found, suggesting it is more the nerve irritation from the tendonitis that is key.
The Journal of Hand Surgery: Journal of the British Society for Surgery of the Hand
Volume 26, Issue 5, October 2001, Pages 475-480
CARPAL TUNNEL SYNDROME: THE CORRELATION BETWEEN OUTCOME, SYMPTOMS AND NERVE CONDUCTION STUDY FINDINGS
L. LONGSTAFFf1, R. H. MILNER, S. O’SULLIVAN and P. FAWCETT abstract here
The Predictive Value of Electrodiagnostic Studies in Carpal Tunnel Syndrome
Concannon, Matthew J. M.D.; Gainor, Barry M.D.; Petroski, Gregory F. M.S.; Puckett, Charles L.
abstract here
3) The feet are something you stand on versus the hands so the foot tarsal tunnel sydrome would be a totally different animal from carpal tunnel.
There are “experts” out there that pretend that tarsal tunnel syndrome in diabetic peripheral neuropathy rarely exists. Yet there is a growing list of studies showing foot/ankle tarsal tunnel release surgery helps Diabetic numbness and helps prevent leg ulcers.
What about tarsal tunnel?

It is entrapment around the ankle similar to carpal tunnel. There are metabolic changes that occur in Diabetics(DM) that predispose to entrapment – much like seen in the increased incidence of carpal tunnel in DM patients. Pressing the area in question should be sore (from the tendonitis). – just behind and below the medial ankle bump. It would be very nice if you could also elicit a tingling down in to the foot/ankle when pressing – something called the tinel’s sign.

A full description of tarsal tunnel syndrome can be obtained from the site I used the above picture from:
http://www.myfootshop.com/detail.asp?Condition=Tarsal%20Tunnel%20Syndrome
Criteria for surgery in Diabetics has been:
1) Symptomatic peripheral neuropathy
2) Tinels sign over the trasal tunnel
The following studies have all demonstrated not only relief of symptoms, but also prevention of diabetic foot ulcers:
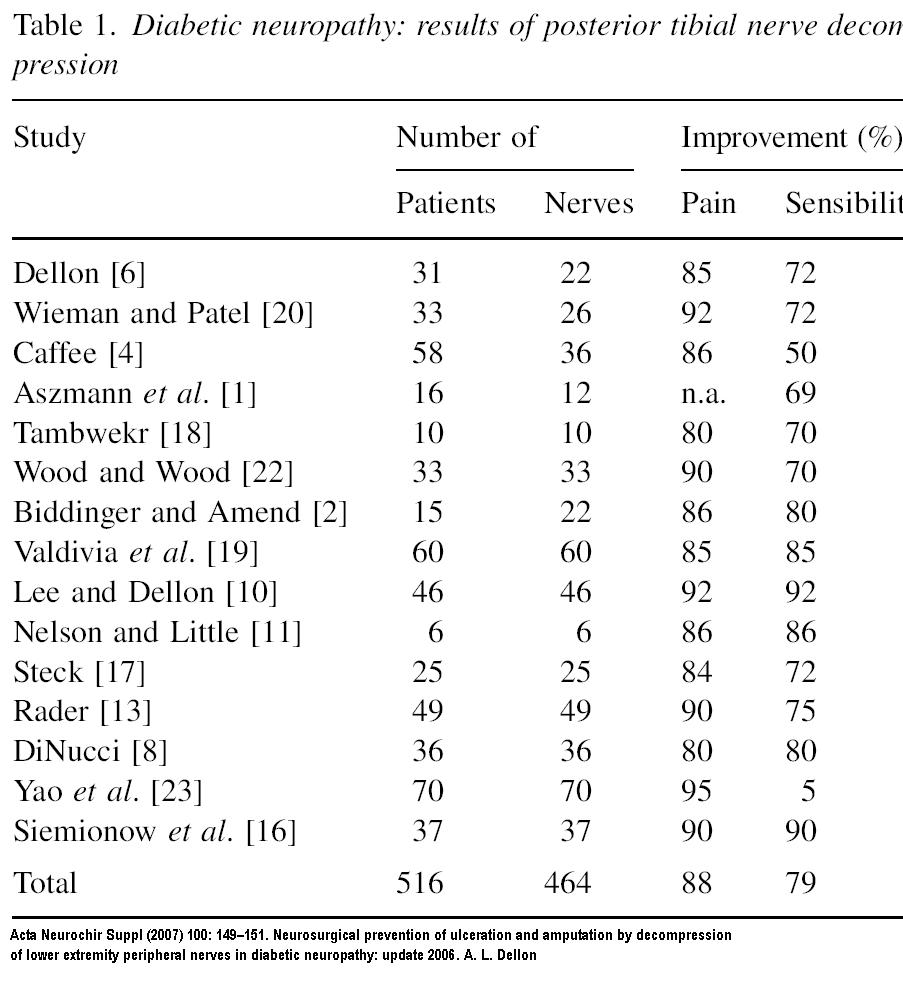
6 – Dellon AL (1992) Treatment of symptoms of diabetic neuropathy by peripheral nerve decompression. Plast Reconstr Surg 89: 689–697 abstract
20 – Wieman TJ, Patel VG (1995) Treatment of hyperesthetic neuropathic pain in people with diabetes; decompression of the tarsal tunnel. Ann Surg 221: 660–665 free article here
4 – Chaffee H (2000) Decompression of peripheral nerves for diabetic neuropathy. Plast Reconstr Surg 106: 813–815 abstract
1 – Aszmann O, Kress KM, Dellon AL (2000) Results of decompression of peripheral nerves in diabetics: a prospective, blinded study. Plast Reconstr Surg 106: 816–821 abstract
18 – Tambwekar SR (2001) Extended neurolysis of the posterior tibial nerve to improve sensation in diabetic neuropathic feet. Plast Reconstr Surg 108: 1452–1453 abstract
22 – Wood M, Wood W (2003) Decompression of peripheral nerve for diabetic neuropathy in lower extremity. J Foot Ankle Surg 42: 268–275 abstract
2 – Biddinger KR, Amen KJ (2004) The role of surgical decompression for diabetic neuropathy. Foot Ankle Clin N Amer 9: 239–254 abstract
19 – Valdivia JMV, Dellon AL, Weinand MD, Maloney CT Jr (2005) Surgical treatment of peripheral neuropathy: outcomes from 100 consecutive decompressions. J Amer Pod Med Assoc 95: 451–454 abstract free article
10 – Lee C, Dellon AL (2004) Prognostic ability of Tinel sign in determining outcome for decompression surgery decompression surgery in diabetic and non-diabetic neuropathy. Ann Plast Surg 53: 523–527 abstract
11 – Nelson SC, Little ER Jr (2006) Pilot study of the use of the SF 36 questionnaire outcome evaluation for multiple lower extremity nerve decompressions in diabetic peripheral neuropathy. J Amer Pod Med AssocJ Am Podiatr Med Assoc. 2007 Mar-Apr;97(2):121-5. abstract
17 – Steck J (2005) Results of decompression of lower extremity peripheral nerve for treatment of symptomatic neuropathy, Presented at Am Soc Peripheral Nerve Meeting, Puerto Rico
13 – Rader A (2005) Surgical decompression in diabetic neuropathy. J Amer Pod Med Assoc 95: 446–450 abstract
8 – DiNucci K (2005) Results of decompression of multiple lower extremity peripheral nerves in diabetic with symptomatic neuropathy, Presented at the Amer College of Foot and Ankle Surgery meeting, New Orleans
23 – Yao Y, Wang RZ, Shang B, Liu FY, Wei UK (2005) Treatment of symptomatic diabetic peripheral neuropathy by surgical decompression of three peripheral nerves. Chin Med J 242: 35–37
16 – Siemionow M (2006) Clinical outcome of peripheral nerve decompression in diabetic and non-diabetic peripheral neuropathy.Ann Plast Surg. 2006 Oct;57(4):385-90. abstract
Since that review there has been more:
Ducic I, Taylor NS, Dellon AL. Relationship between peripheral nerve decompression and gain of pedal sensibility and balance in patients with peripheral neuropathy. Ann Plast Surg. 2006;56:145–150. abstract
What this analysis showed was that pain improved by 88% and sensation improved 79%.
A more recent review:
Annals of Plastic Surgery: August 2009 – Volume 63 – Issue 2 – pp 217-221
Nerve Decompression Surgery as Treatment for Peripheral Diabetic Neuropathy: Literature Overview and Awareness Among Medical Professionals
Melenhorst, Wynand B. MD; Overgoor, Max L. MD; Gonera, Ed G. MD; Tellier, Michiel A. MD; Houpt, Peter MD, PhD
They discuss the lack of control groups which is thought of as unethical:
“Finally, the most important criticism regards the lack of proper control groups, in which study subjects do not undergo surgery. Three of the studies form an exception, as these included an
alternative control: surgical decompression in 1 of 2 affected nerves within the same patient, with postoperative comparison of the 2 sides. In the first study from 1992, patients with diabetes (n =60) with symptoms of PDN were prospectively included to undergo surgical decompression of 154 nerves in elbow, forearm, wrist, knee, ankle, and foot.33 Intriguingly, with a mean follow-up of 30 months, improvement of neuropathy of the decompressed side was 100% for patients with localized nerve compression, 80% for neuropathy with superimposed nerve compression and 50% for diffuse neuropathy. Importantly, the untreated nerves showed neuropathy worsening in 50%. Despite absence of control groups and the performance of various unrelated nerve decompressions, this study clearly demonstrates the potential of decompression surgery to
change the natural course of PDN. In a second study, 12 patients with PDN, pre- and postoperatively assessed for 2-point discrimination, underwent surgical decompression of the posterior tibial nerve.24 Sensory function improved in 69% of operated nerves, whereas neuropathy of nonoperated contralateral nerves remained unchanged in 59% and progressed in 32%. Although the number of treated patients is small, the differences between treated and untreated nerves within one patient illustrate the potential of nerve decompression surgery. Third, a retrospective case study reviewed 50 patients with diabetes with PDN who underwent unilateral
surgical decompression of the peroneal or tibial nerve.23 With a mean follow-up of 4.5 years, no ulcers or amputations had occurred in surgically decompressed sides, whereas nonoperated sides developed 12 ulcers and 3 amputations. Despite its retrospective nature, this study demonstrates the potential of decompression surgery to reduce PDN-related morbidity.”
With the age of evidence based medicine (gag) people have decided to ignore overwhelming evidence because a randomized control trial has not been done.
This includes
- Cochrane
Cochrane Database Syst Rev. 2008 Jul 16;(3):CD006152.
Decompressive surgery of lower limbs for symmetrical diabetic peripheral neuropathy.
Chaudhry V, Russell J, Belzberg A. abstract
“MAIN RESULTS: This review failed to identify a single randomized controlled trial or any other well designed prospective study controlling for the non-operated limb that showed improvements in pre defined end points after decompressive surgery. AUTHORS’ CONCLUSIONS: The results of this review suggest that the role of decompressive surgery for diabetic symmetric distal neuropathy is unproven.”
- Neurology
NEUROLOGY 2006;66:1805-1808
Practice Advisory: Utility of surgical decompression for treatment of diabetic neuropathy
Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology Vinay Chaudhry, MD, James C. Stevens, MD, John Kincaid, MD and Yuen T. So, MD, PhD
abstract
“Given the current evidence available, this treatment alternative should be considered unproven (Level U). Prospective randomized controlled trials with standard definitions and outcome measures are necessary to determine the value of this therapeutic intervention. ”
———
A full (and I mean full – a thesis) description of the surgery and related surgery can be found free here
Doctors rarely even mention this form of treatment.
In:
Annals of Plastic Surgery: August 2009 – Volume 63 – Issue 2 – pp 217-221
Nerve Decompression Surgery as Treatment for Peripheral Diabetic Neuropathy: Literature Overview and Awareness Among Medical Professionals
Melenhorst, Wynand B. MD; Overgoor, Max L. MD; Gonera, Ed G. MD; Tellier, Michiel A. MD; Houpt, Peter MD, PhD
They sent out a questionaire and these were the results (sorry didn’t show well:
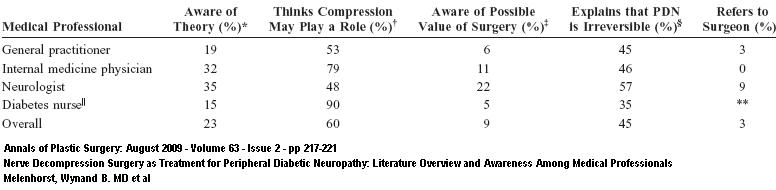
Basically states that only 5-22% of doctors aware surgery might help.
Comment – Innocently, I came across a recent Turkish article describing favorable results of decompression surgery. 1 year ago. I mentioned this to the Neuropathic Pain Group – Canadian Pain Society 2008 meeting in Victoria, BC – when they found the article was from Turkey, the whole issue itself was ignored and I was literally laughed away. Yesterday, I was at a talk on diabetic neuropathy, and the issue of entrapment was received with groans. The neurologist was nice enough to mention he sends people for steroid injection of the tarsal tunnel as a diagnostic technique and takes it from there.
Injection technique is simple:
1) Find where tinel’s sign is and go 2 cm proximal. Aim distal – 30 degrees to skin. inject superfically and laterally to nerve where tibialis posterior is.
Use 3-6 mls with 40 mg kenalog and local.

Discussion of injection:
AAFP – here
Fnotebook – here
In my town, I have never heard of anyone having tarsal tunnel surgery. My personal feelings is that there are a lot of block heads out there that ignore the fact that chronic pain causes considerable peripheral sensitization and that produces multiple pain generators.
Addendums:
See followup articles:
Nerve Entrapment in Diabetic (DM) Peripheral Neuropathy – Surgery Helps Foot Ulcers and Charcot Foot Syndrome
Electrodiagnostically, Tarsal Tunnel Syndrome Rampant in Diabetics
Chronic Severe Pain – For Gd’s Sake Don’t Forget Peripheral Pain Generators
Any comments?
Pingback: Severe Neuropathic Pain – Only 1/4 Respond to Standard Drug Protocols – What Else Is There? | Pain Medical Musing
Hello,
My fiance has diabetic peripheral neuropathy in his foot on the outside of the foot and he has it also in his big toe on the right side and suffers severely with it. I believe he is one of the most advanced cases I have ever read about. His pain levels get up to 7 or 8 on the pain level scales. So is there someone out there who has had the surgery for this kind of neuropathy let me know your out come and if it helped your pain at all. We are in desperate need of some pain relief for him. We have been prescribed every kind of medicene there is out there to use that has been approved for diabetic Peripheral neuropathy. We have used Gabapentin, oxycodone, oxycontin, Moriphine, Cymbalta, Lexapro, Ecitalopram and many more of which none have worked for him in the least. We have used all kinds of things that doctors have told us to use like capsacin cream, lidicaine cream, vitamin B creams, Aloe vera cream cream, you name it we have tried it. I have even seen him cry from the severe pain he suffers from it. Anyone can you help us. We were told that there is no such surgery for diabetic Neuropathy. We are at our witts end and I fear that he might do something to himself some day because he can’t take the pain anymore. He says he wouldn’t but you just never know what pain will do to a persons mind once they can’t take anymore and decide to give up. Thanks to all who read my post and if you can help us God Bless You all, and have a pain free day
________________
-consider that there may be local problems that are aggravating it; a bone scan might highlight that. If circulation is an issue, then an angioplasty (stent) might help.
-Lateral foot pain can come from a “dropped” cuboid even with other issues present:
“Two examples of ‘cuboid syndrome’ with active bone pathology: Why did manual therapy help.” Mark Lewis et al. Manual Therapy 19 (2014) 494-498.
http://www.sciencedirect.com/science/article/pii/S1356689X1300194X`
I had started a wiki on diabetic neuropathy but never finished it:
It is available here:
http://wiki.painmuse.org/index.php/Diabetic_Neuropathy
Things I have been using include:
– Near daily shots of B12 – my daughter and I poster published results of it for pain and found about a 20%+ reduction in pain – it augments gabapentin/lyrica too. Oral B12 can give some results but took much longer.
http://wiki.painmuse.org/images/e/ee/B12_dn.png
– Caudal (tailbone epidurals) of vitamin B12 and 5% dextrose – discussed in wiki
– COMBINATION THERAPY of venlafaxine (Effexor) or Cymbalta and pregabalin (lyrica) – I know, you have tried them separately – but combos work better and you do not have to take “toxic” doses of either of them
– tramadol or opioids (don’t expect huge improvements from painkillers)
– inject tender nerve tracts with sugar water (D5W) – called neural prolotherapy
For severe cases, spinal stimulation is a new option:
http://bja.oxfordjournals.org/content/early/2012/08/13/bja.aes251.full
Methadone has been suggested to give pain relief:
http://care.diabetesjournals.org/content/28/2/485.full.pdf