
TNF-alpha Modulation for Treatment of Alzheimer’s Disease: A 6-Month Pilot Study.
MedGenMed. 2006 Apr 26;8(2):25.
Tobinick E, Gross H, Weinberger A, Cohen H Abstract
full
Comment – Looks like Etanercept (Embrel) works as well as Aricept in a 6 month pilot study in preventing AD progression. This suggests inflammatory disease is involved in AD disease. It has been suggested that some chronic pain involves the same mechanism.
Inflammation has been confirmed in Fronto-Temporal Dementia: Abstract
Full
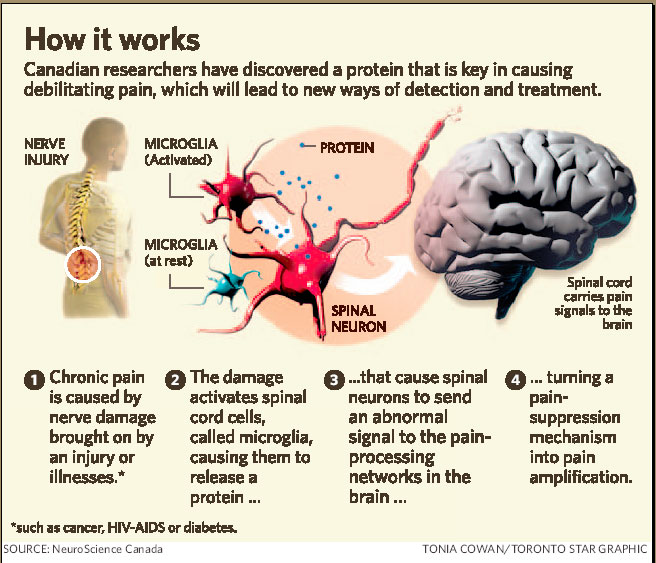
What causes significant inflammation in the brain and how do you treat it? This inflammation is mediated thru Glial cells:
{kind=link}
link to review CRPS includes all references: Full
1)Chronic pain:
Pain. 2005 Aug;116(3):213-9. Changes in cerebrospinal fluid levels of pro-inflammatory cytokines in CRPS. Alexander GM, van Rijn MA, van Hilten JJ, Perreault MJ, Schwartzman RJ.
Though TNF did not appear to be one of the inflammatory compounds elevated there. But does for neuropathic pain:
Brain Res. 1999 Sep 11;841(1-2):70-7. Brain-derived TNFalpha mediates neuropathic pain. Ignatowski TA, Covey WC, Knight PR, Severin CM, Nickola TJ, Spengler RN
2) Ischemic brain injury Abstract
3)Stress – subjects with Irritable bowel being inordinately susceptible: Abstract
4) Autoimmune disease
5) Obesity 6) Depression 7) Atopy/Allergy
8) Atherosclerosis
9) Infections and even Vaccinations 10) ?Sleep
11) B12 Deficiency: Abstract
12) Magnesium deficiency:
13: Clonidine – worked in acute perioperative setting:
Abstract
Take a subject with chronic pain. Obese due to inactvity due to pain. Sleep disturbance and depression due to pain. That would make them sitting ducks for AD.
Cytokines are getting much more respect as they are implicated in Beta cell destruction in the pancreas of diabetics (BYW the same pathological changes seem in AD have been recently seen in the pancreas). Cytokine reactions might play a major role in the deaths with the “duck flu” and discussion is raging how cytokine agents might be the only defense.
Potential treatments for inflammation:
1) Vitamin C – reduced oxidative stress endothelial dysfunction in intermittent claudication: Abstract
Low Vit C levels can predict unstable angina – might suggest angina patients take more Vit C: Abstract
B6 and Vitamin C levels relate to Carpal tunnel: Abstract
Vit C supplementation cut Reflex Sympathetic Dystrophy/CRP Syndrome rates following wrist fracture from 22% to 7%: Abstract
link to review CRPS includes all references: Full
Cochrane review indicates Vitamin C modest effects on colds, particularly under body stress conditions (cold environments, extreme exercise): Abstract
Ascorbic acid levels under 2.5 mg/l is deficient.
2) B12 and Magneium – if low – supplement + maybe check for celiac. Check Magnesium levels not very accurate given that most is intracellular.
3) NSAIDS – Patients with RA should have high AD levels but don’t. Unfortunately, the truly beneficial ones in AD must inhibit beta-amyloid42 production – only Indomethacin, Sulindac and Ibuprofen do so (NOT Naproxen, Diclofenac nor Celebrex).
4) Statins: – reduce inflammation of arteries and brain:
Abstract
Simvastatin 80 mg/d reduced MS plaque by 44% in 6 months:
Abstract
Interestingly, fluvastatin (Lescol)(fat soluble) helps treat Rheumatoid arthritis but through its ablitity to kill Synovial cells (but not Pravastatin – water soluble):
Full
5) Minocycline – is a glia cell inhibitor. Glial cells are a very hot topic and a implicated in causing central brian damage and sensatization, and spinal cord central sensitization.
Abstract
Minocycline appears helpful in Rheumatoid arthritis: Abstract
6) Leflunomide and Methotrexate – used in Rheumatoid arthritis.
7) Thalidomide:
Rajkumar, S. V., Fonseca, R. & Witzig, T. E. Complete resolution of reflex sympathetic dystrophy with thalidomide treatment. Arch. Intern. Med. 161, 2502–2503 (2001).
Prager, J., Fleischman, J. & Lingua, G. Open label clinical experience of thalidomide in the treatment of complex regional pain syndrome Type 1. J. Pain 4 S68 (2003)
8) TNF inhibitors – Infliximab, Anakinra (Kineret; Amgen), Etanercept (Enbrel; Amgen/Wyeth)
9)Ketamine: Full
10) Ace Inhibitors?? Abstract
Another issue is the fact that chronic pain is in part a degenerative disease – due to the degeneration of the decending inhibitory circuits for pain control. This is apparently why shingles is so much more painful in the elderly. But that is another story…
I would be interested in any comments on using glial cell/inflammatory inhibitors in chronic pain. Minocycline seems promising but then you have to worry about Lupus-like syndrome and pseudotumor cerebra headaches among other things ( Have seen cholestatic jaundice). Our drug plan will not cover it. Statins might be another but they seem to be not all created equal…
ADDENDUM:
Cases of Tumor Necrosis factor Inhibitor Etanercept (Enbrel) associated with improvement in dementia since this was first written:
1) Neuroinflammation. 2008; 5: 2.
Rapid cognitive improvement in Alzheimer’s disease following perispinal etanercept administration
Edward L Tobinick1,2 and Hyman Gross
abstract:
- Substantial basic science and clinical evidence suggests that excess tumor necrosis factor-alpha (TNF-alpha) is centrally involved in the pathogenesis of Alzheimer’s disease. In addition to its pro-inflammatory functions, TNF-alpha has recently been recognized to be a gliotransmitter that regulates synaptic function in neural networks. TNF-alpha has also recently been shown to mediate the disruption in synaptic memory mechanisms, which is caused by beta-amyloid and beta-amyloid oligomers.
- The efficacy of etanercept, a biologic antagonist of TNF-alpha, delivered by perispinal administration, for treatment of Alzheimer’s disease over a period of six months has been previously reported in a pilot study.
- This report details rapid cognitive improvement, beginning within minutes, using this same anti-TNF treatment modality, in a patient with late-onset Alzheimer’s disease. Rapid cognitive improvement following perispinal etanercept may be related to amelioration of the effects of excess TNF-alpha on synaptic mechanisms in Alzheimer’s disease and provides a promising area for additional investigation and therapeutic intervention.full article here free
2) BMC Neurol. 2008 Jul 21;8:27.
Rapid improvement in verbal fluency and aphasia following perispinal etanercept in Alzheimer’s disease. Tobinick EL, Gross H.
3) review now published considers TNF a gliotransmitter
Drug Discov Today. 2008 Nov 20. [Epub ahead of print] Perispinal etanercept for neuroinflammatory disorders. Tobinick E. Institute for Neurological Research, a private medical group, inc. 100 UCLA Medical Plaza, Suites 205-210, Los Angeles, CA 90095, United States.
Excess TNF is centrally involved in the pathogenesis of a variety of neuroinflammatory disorders, including Alzheimer’s disease, other forms of dementia, intervertebral disc-related pain, and related disorders. TNF causes neuronal dysfunction, regulates synaptic mechanisms, and mediates amyloid-induced disruption of molecular mechanisms involved in memory. Perispinal administration of etanercept, a potent anti-TNF fusion protein, is a treatment modality whose rapid clinical effects may be related to modulation of these TNF-related mechanisms, particularly the role of TNF as a gliotransmitter capable of regulating synaptic transmission. This approach utilizes therapeutic delivery of etanercept across the dura via the cerebrospinal venous system, a confluence of the venous plexuses of the spine and the brain, in which flow is bi-directional owing to the absence of venous valves.