
A Nose pain issue with pain out of control could represent a nasal neuralgia with a treatable injection regimen.
External Nasal Neuralgia
García‐Moreno, Héctor, et al.
External nasal neuralgia: A neuropathic pain within the territory of the external nasal nerve.
Headache: The Journal of Head and Face Pain 55.9 (2015): 1259-1262.
http://onlinelibrary.wiley.com/doi/10.1111/head.12625/full
- potential causes trauma, infection, cancers and unknown “idiopathic rhinalgia”
- idiopathic forms have various names – nasociliary neuralgia (Charlin’s neuralgia)
infratrochlear neuralgia - case 76 yr old lady with 30 year history initially of paroxysms of mild tingling sensation on side of nose – mostly during day
- amitriptyline helps
- changed to severe pains lasting 20-30 minutes occurring 2-3 times a day
- nose was tender and palpation could trigger attack
- tenderest spot was where bone ended and cartilage started
- blood work oncluded EST and CT face was normal
Treatment involves injection:
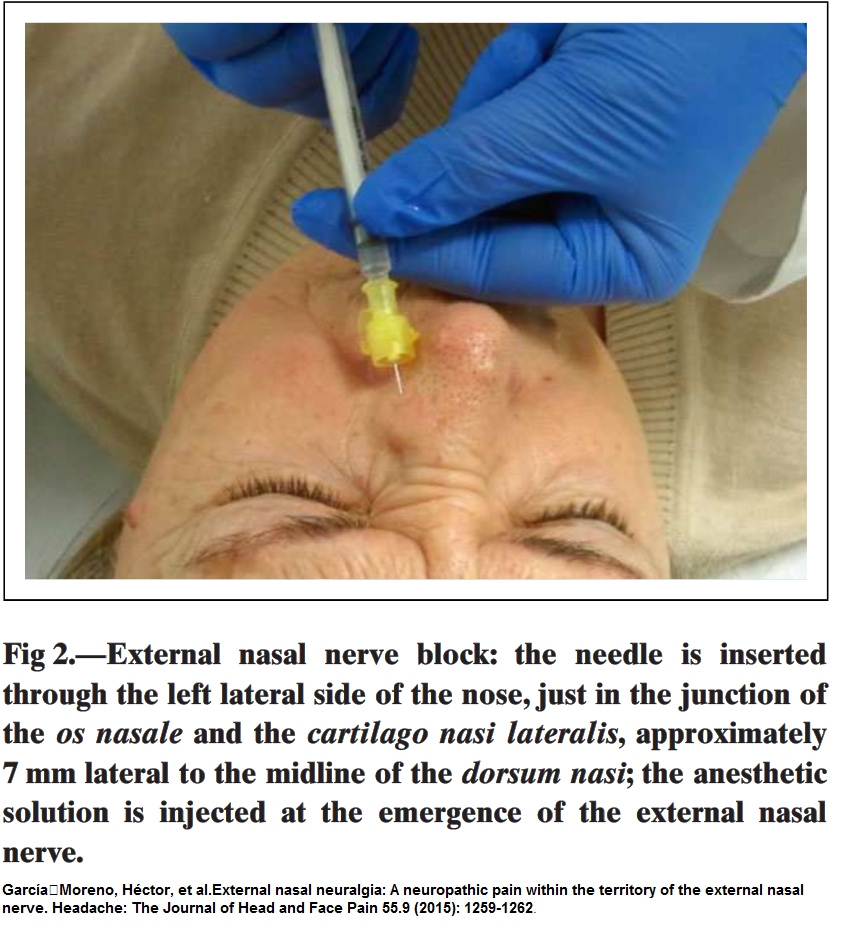
- injections of 0.5 mL of bupivacaine 0.5% with a 30-gauge needle every few months gave relief
- spot where bone ends is the best spot
- used 4% intranasal lidocaine as well
—————————————————–
Another naso-facial neuralgias written up:
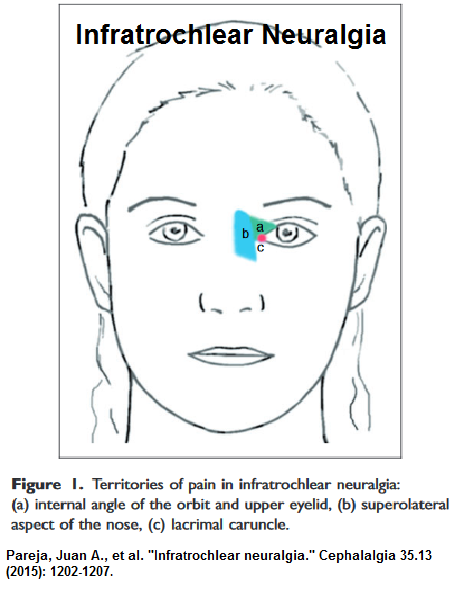
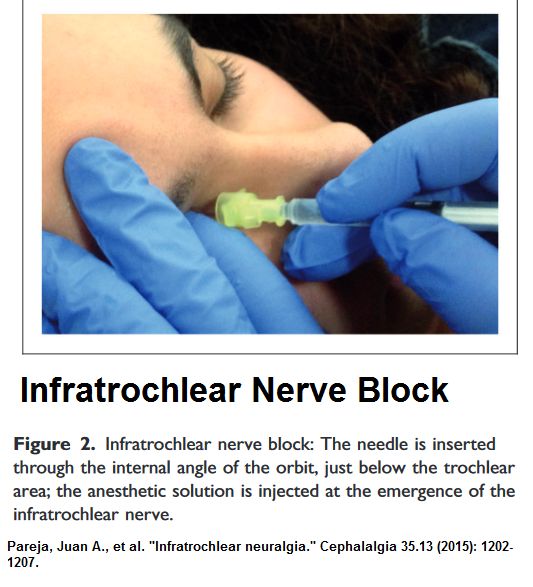
Infratrochlear Neuralgia:
Pareja, Juan A., et al.
Infratrochlear neuralgia.
Cephalalgia 35.13 (2015): 1202-1207.
http://journals.sagepub.com/doi/abs/10.1177/0333102415578429
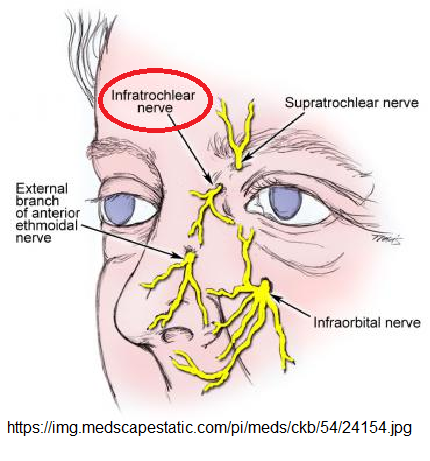
 The Infratrochlear nerve:
The Infratrochlear nerve:
- comes from nasociliary nerve (one of the terminal
branches of V-1) - follows the inferior edge of the superior oblique muscle up to its
pulley - leaves orbit below the trochlea
- feeds the medial aspect of the upper eyelid
- also feeds the bridge of the nose
- also feeds the lacrimal sac and caruncle.
- They excluded eyeglass trauma which one would think is relevant to that location
Tests they thought relevant were:
- ESR, CRP
- “Immunological tests, including quantitative immunoglobulin testing”
- RA factor
- Lupus anticoagulant
- ANA for lupus
- anticardiolipin antibodies
- antithyroid antibodies;
- MRI brain and paranasal sinuses
- Mostly women – 6 female; 1 man
- age average – 46 (13-73)
- problems 1 month 1 2 years
- spontaneous onset
- paroxysmal, shot-like pain
- severe 7+/10
Location fixed to one of 3 locations:
- internal angle of the orbit and upper
eyelid (3) - side of the bridge of the nose (3)
- lacrimal caruncle (1)
Features:
- Pain lasted 5-30 seconds
- daily 1-20 attacks a day
- 2/6 could trigger it with touch
- though random, did not occur at night
- local excessive tenderness
Treatment:
- Gabapentin ( most on 900 mg/day) worked well in all cases and was able to be stopped in 2-6 months
- one underwent remission with injection – “injecting 0.5 cc of bupivacaine 0.5% with a 30-gauge needle through the internal angle of the orbit, just below the trochlear area”
 Comment – you see what you know – and injection or gabapentin seems to be the ticket
Comment – you see what you know – and injection or gabapentin seems to be the ticket
Post‐Traumatic External Nasal Pain Syndrome
In real life, post-traumatic nasal pain cases are much more complicated:
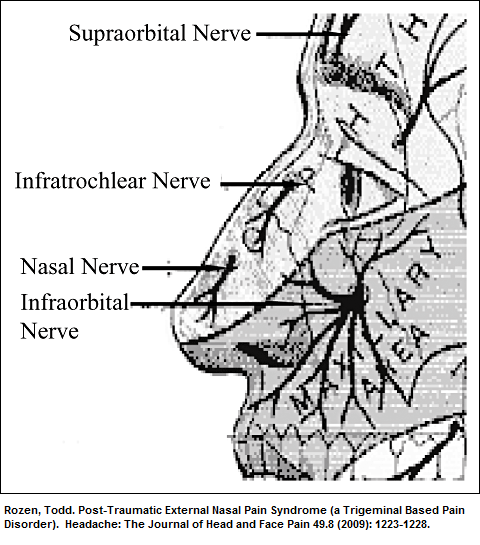
Rozen, Todd.
Post‐Traumatic External Nasal Pain Syndrome (a Trigeminal Based Pain Disorder).
Headache: The Journal of Head and Face Pain 49.8 (2009): 1223-1228.
http://onlinelibrary.wiley.com/doi/10.1111/j.1526-4610.2009.01485.x/full
 Article presents 4 cases with variety of nerve involvements
Article presents 4 cases with variety of nerve involvements
1 – pregabalin 675 mg worked well
2 – snorkeling injuries –
- daily pain “on both sides and the bridge of his nose” – became extremely disabled
- bilateral supratrochlear, infraorbital and bilateral maxillary nerve blocks only gave short term results.
- Left sphenopalatine ganglion block gave good relief so had left sphenopalatine ganglion rhizolysis, which made his pain >75% improved.
- Surgical treatment of deviated septum with contact point helped gain good control
3 – lady with pain and sensitivity whole nose after an assault. –
- local blocks were short term and botulinum minimally effective.
Point here – I find botulinum injections in neuropathic pain softens up the nerve to blocks especially treatment with semineurolytic agents like 5-10% lidocaine. So just expecting botulinum to work is too much to expect but a combo use gets good results.
- As it was, she then had excellent response to several nerve blocks.
- Not realizing why the results of the combo worked well, they went on a different tack to sphenopalatine rhizotomy which worked for 1 year.
- Following that, had right maxillary nerve pulsed radiofrequency with some relief.
- Then had bilateral infratrochlear blocks and then pulsed radiofrequency of the infratrochlear nerves with good results.
Goes to show that perseverance pays off
4 – 14 yr old with bridge nose and bilateral lateral portions
- worse with valsalva and exercise. May have had trauma from repeatedly “heading” ball playing soccor
- got bad enough for hospitalizations twice
- had a persistent component and a severe overlying part
- regimens for migraine include IV were ineffective
- supraorbital and supratrochlear blocks failed; infratrochlear blocks short lived with rebound pains
- botulinum failed
- trigger injections failed
- nasal contact surgery failed
- memantine 30 mg gave good relief for past 2 years and flares were handled by “short dexamethasone taper”
- sphenopatine block was considered but costs prevented it
wow – hurray for memantine
Comment – What I got from these articles is:
- Know your nerves and where to block but if you are serious about a nerve you need to consider rhizotomy
- Botulinum PLUS subsequent nerve blocks might help but botulinum alone is rarely effective
- Nasal contact surgery might help if septum deviated enough to contact side of nose – helped 1/2 of time (in 2 cases so far)
- Sphenopalatine block worth using and if successful, subsequent rhizotomy is an alternative
- Pregabalin higher dose, and memantine might be worth a try