
Opioid deaths seem to be fueling more by Chinese derived illicit fentanyl. However, massive efforts are made to lower opioid dose. One study was successful at getting opioid consumption down from 288 mg to 150 mg. They weren’t any better for it despite the theoretically “dangerous high levels” which would probably not be a problem if they avoided chinese imports. There was no effort to have a control group to see how many more deaths there were in the “dangerously high” group.
I have not had much luck tapering opioids and a recent analysis explains why. They claim opioids are integrated in mood, energy, motivation, social functioning and personality systems and withdrawing doses will effects all of it. Above study was successful because they started with 5% reductions in the first month and upped it to 10% every 2 weeks in the second month.
Darnall, Beth D., et al.
Patient-Centered Prescription Opioid Tapering in Community Outpatients With Chronic Pain.
JAMA Internal Medicine 2018 in press
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2672574
- average 51 years, and 60% were women
- They made NO effort to have a control group so there is no information on what happened to those on dangerously high doses – though I suspect nothing happened.
- average initial opioid dose was 288 morphine equivalents
- A whopping 38% dropped out of study making me wonder why the continued with study as all you will see are the results of a hardy, determined, stable bunch
- “Opioid dosages were reduced up to 5% for up to 2 dose reductions in month 1 to minimize negative physical and emotional response, withdrawal symptoms, and to facilitate patient confidence in the process. In months 2 to 4, patients were asked to further reduce use by as much as 10% per week; dose decrements were tailored to the patient.”
– now, you are not going to find long acting formulations in this 5% reduction range so they would have had to fake it with short acting pills interspersed - 4 month study – got people down to 150 mg morphine equivalents
- They looked at pain interference based on the Patient Reported Outcomes Measurement Information System (PROMIS) questionnaire;
It looks at functioning in the following areas: (based on analysis of short form
Measurement equivalence of the Patient Reported Outcomes Measurement
Information System (PROMIS) Pain Interference short form items: Application
to ethnically diverse cancer and palliative care populations
Jeanne A. Teresi et al
Psychological Test and Assessment Modeling, Volume 58, 2016 (2), 309-352
http://www.psychologie-aktuell.com/fileadmin/download/ptam/2-2016_20160627/05_Teresi.pdf
- life enjoyment
- concentration
- activities
- recreational enjoyment
- tasks away like groceries
- participate in social activities
- work at home
- usual fun things
- fun with social activities
- how often pain prevents socializing
- pain average
There was NO IMPROVEMENT in pain, functioning, concentration, enjoyment etc.
Yes that’s right NO DIFFERENCE. So people were put thru the suffering of withdrawal to end up no better. You would have thought taking less opioids would have helped concentration but apparently not. They were taking less “dangerous opioids” without showing the dangerous effects on a control group which BTW I suspect were none. They attempted to made the process look easy without explaining the 38% drop out rate.
Several parts of this study I find very objectionable
The high drop out rates reminds me of a key study that found opioids work very well:
Watson, C. Peter N., et al.
Controlled-release oxycodone relieves neuropathic pain: a randomized controlled trial in painful diabetic neuropathy.
Pain 105.1-2 (2003): 71-78.
https://pdfs.semanticscholar.org/be4f/ff311b5869e11245dbc5ed433e59035d0f9c.pdf
look at their drop out rates
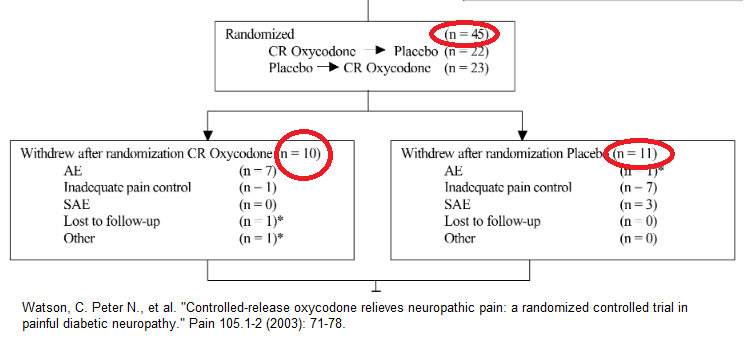 So results were based on a subgroup who did well on opioids and made it look worthwhile. Better followup studies showed that opioids with out the placebo effect on average only drop pain by 1/10 but this study helped fuel the opioid epidemic.
So results were based on a subgroup who did well on opioids and made it look worthwhile. Better followup studies showed that opioids with out the placebo effect on average only drop pain by 1/10 but this study helped fuel the opioid epidemic.
Now, we have a similarly biased study to help fuel the opioid reduction epidemic. G’d help me – do we ever learn?
The fact that these people were not functioning any better is a big disappointment for all the work put into finding 5% decrements on people on long lasting pills that do not have 5% decrements. There might be a financial saving and I guess for those not on assistance that is something.
Those that did well? – those on marijuana (p=0.04). This substance is about to become legal in our country and I believe might blunt our opioid epidemic but may open a can of worms…
Depression interfered (p=0.05). I do not put depressed subjects on smoking cessation and that seems plausible for opioid reduction as well.
Comment – more of a plus for a hardy group and marijuana use which seems to make opioid reduction easier. Don’t expect to feel any better….
Why is it so difficult to taper? Recently publish commentary adds a perspective:
Hijacking the endogenous opioid system to treat pain: who thought it would be so complicated?
Daniel Clauw
Pain December 2017. 158(12) 2283-4
https://journals.lww.com/pain/Citation/2017/12000/Hijacking_the_endogenous_opioid_system_to_treat.3.aspx
It is contended that the opioid system is linked to fatigue, mood, motivation, social engagement and personality. Reducing dose effects all these systems. That would explain my lack of results even with determined people to cut dose. Now there is even less evidence it is worthwhile. Am thinking more about marijuana use though as a mechanism to gain relief and lessen dose from an agent that does not work very well.
I would be interested in comments as this is a difficult topic.
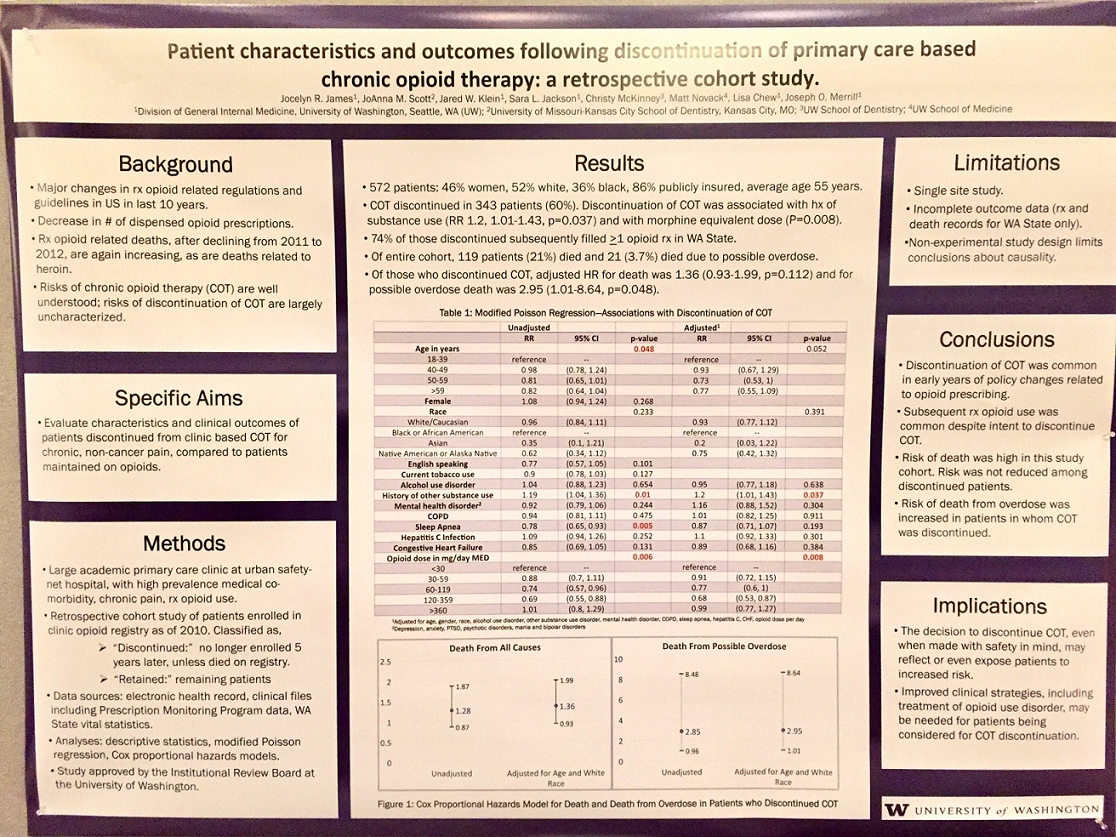
Addendum _ It gets worse when practitioners no longer prescribe opioids:
Patient characteristics and outcomes following discontinuation of primary care based chronic opioid therapy: a retrospective cohort study
Jocelyn James et al. Uni. Washington
Poster April 2018
- death rates from Washington state – just south of BC:
“Risk of death from overdose was increased in patients in whom COT [chronic opioid therapy] was discontinued”
so stopping opoiods does not decrease death rates, it increases it.
(click on it to see bigger)
 [https://pbs.twimg.com/media/Dat7e5jVQAEzpae.jpg]
[https://pbs.twimg.com/media/Dat7e5jVQAEzpae.jpg]