
Less than 30% patients respond to antidepressants. Study cataloged depression scale and other features and came up with predictors of depression response particularly to Escitalopram. They included Demographics like black, unemployed, and uneducated; Depression severity and persistence all day ; Longstanding issues with depression; PTSD symptoms; Anxiety attack fear avoidance; Sleep issues, and some miscellaneous issues like Insight into depression, Energy issues, Psychomotor agitation, and widespread aches and Pains. People with those features would respond to SSRI’s like Escitalopram. Otherwise SNRI’s like venlafaixine or mirtazepine would be more effective.
Cross-trial prediction of treatment outcome in depression:a machine learning approach
Adam Mourad Chekroud, Ryan Joseph Zotti, Zarrar Shehzad, Ralitza Gueorguieva, Marcia K Johnson, Madhukar H Trivedi, Tyrone D Cannon, John Harrison Krystal, Philip Robert Corlett
The Lancet Psychiatry 2016 in press
http://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366%2815%2900471-X/abstract
- Data mined 164 variables in 665 patients.
- Came up with 25 variables:
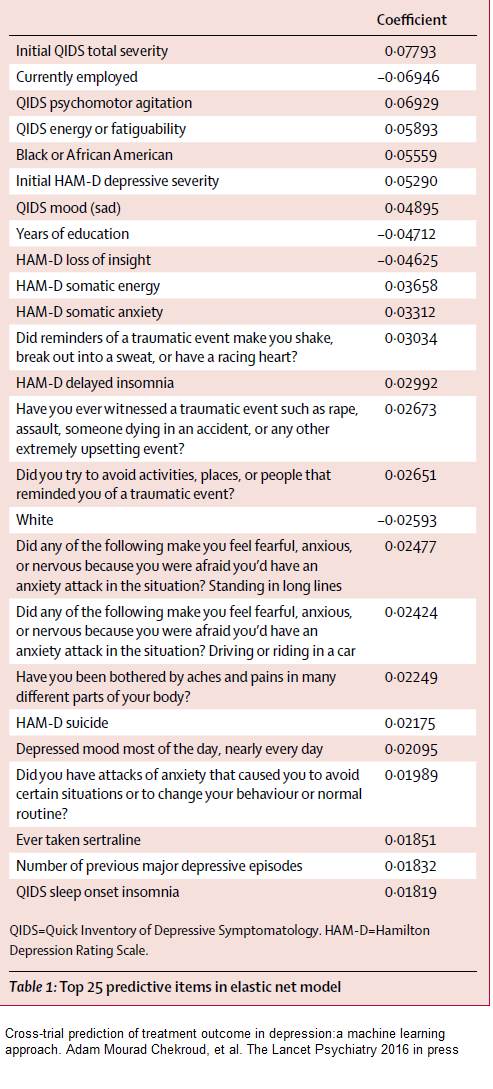 I have tried to put them into a form of checklist:
I have tried to put them into a form of checklist:
Race:
Black
Not white
Demographic:
Unemployed
Poor education
Depression:
Severe
Suicidal
Unrelenting (most of day)
Prior episodes
Sertraline use prior
PTSD symptoms:
Witness rape, assault, accident or other traumatic very unsettling event
Trigger response – reminders cause shaking, sweating, or heart pounding
Avoidance – avoid activities, places, people reminders of trauma
“Anxiety Attack” Fears:
Fear of standing in long lines re trigger anxiety attack
Fear driving/riding in car re anxiety attacks
Avoid situations/routines/behaviors for fear anxiety attack
Sleep issues:
Sleep onset insomnia
Delayed insomnia
Miscellaneous:
Insight into depression
Lack of energy
Psychomotor agitation
widespread aches and pains
I have made this into a word checklist:
depression_predict
Comment:
Many of these features are more bipolar/major mood disorder features:
- Severe all day
- Suidical
- longterm
- Anxiety – typically the comorbidity of anxiety greatly ups the possibility it is bipolar
- PSTD
- Insomnia – I have bipolar cases that felt they have never slept well
- Psychomotor agitation – that’s a hypomanic/mixed state feature
- fatigue, widespread pains – recent article found 20% of Fibromylagia patients have bipolar disorder
- I presume chronic depression causes poor education (adolescent turmoil, drop out and maybe drugs), and poorer employment but sometimes the exact opposite is true…
This group may respond to Escitalopram though in some cases they augmented it with bupropion (Wellbutrin). Reviewer of article was skeptical this would change anything but it just heightens my suspicions in chronic depressed pain patients. People with dumbed down depressions I will give more Venlafaxine (Effexor) or Mirtazepine (Remeron). I am reluctant to start bipolar like patients on straight antidepressants for fear of Bipolar type III reactions – pushing them into a hypomanic or mixed state – and at least I have them on quetiapine for sleep first and maybe some risperidone.