
After a car accident, TOS can pinch nerves in the neck and cause neck and arm pain with arm/hand numbness that nobody can seem to find a reason for. A simple injection into the anterior scalene muscle can prove the source and Botulinum injection some relief
Pain Med. 2010 Mar 1. [Epub ahead of print]
Single CT-Guided Chemodenervation of the Anterior Scalene Muscle with Botulinum
Toxin for Neurogenic Thoracic Outlet Syndrome.
Christo PJ, Christo DK, Carinci AJ, Freischlag JA. abstract here
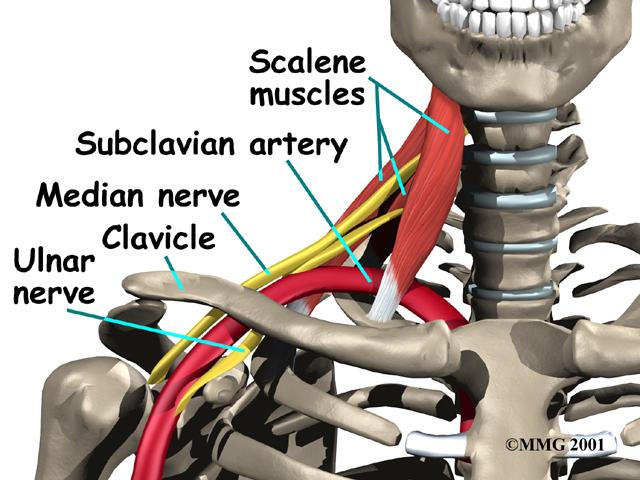
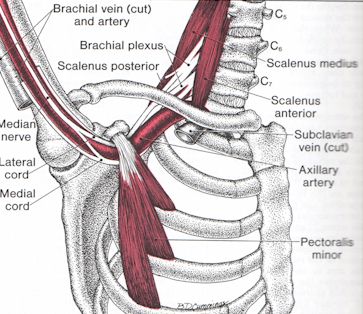
Scalene based Thoracic outlet syndrome is where the arm nerves are caught up in neck scalene spasm:
Post Whiplash Condition
This condition is common after a Motor Vehicle Accident as found by this Canadian study:
Clin J Pain. 1995 Dec;11(4):316-24.
Thoracic outlet syndrome after motor vehicle accidents in a Canadian pain clinic population.
Mailis A, Papagapiou M, Vanderlinden RG, Campbell V, Taylor A. abstract here
Criteria and Testing
Criteria for condition include:
1) Symptoms initiated or aggravated by having arms elevated over head.
2) Numbness hand – especially the outer fingers
3) Tenderness above the clavicle (supraclavicular) where the arm nerves come out between scalene.
4) Positive Roos test – arms up, abducted, externally rotated and back.
(tests as mentioned in:
Manual Therapy 14 (2009) 586–595.
Thoracic outlet syndrome part 1: Clinical manifestations, differentiation and treatment pathways.
L.A. Watson et al)
The Roos test is done with hands in the “hold up” position held for 3 minutes.
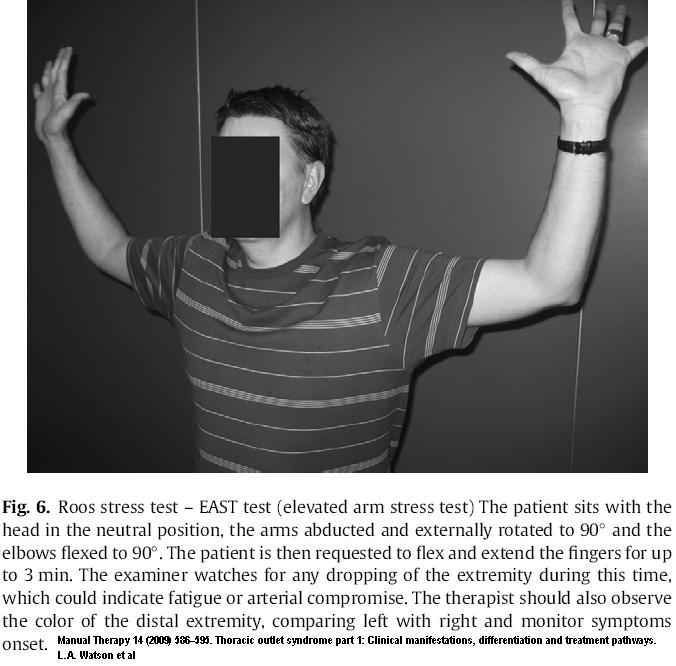
It is considered highly sensitive to all causes of TOS but does have problems with specificity as 58% of people with carpal tunnel syndrome can be positive (though carpal tunnel not positive in Adson test (<5%)) (below)
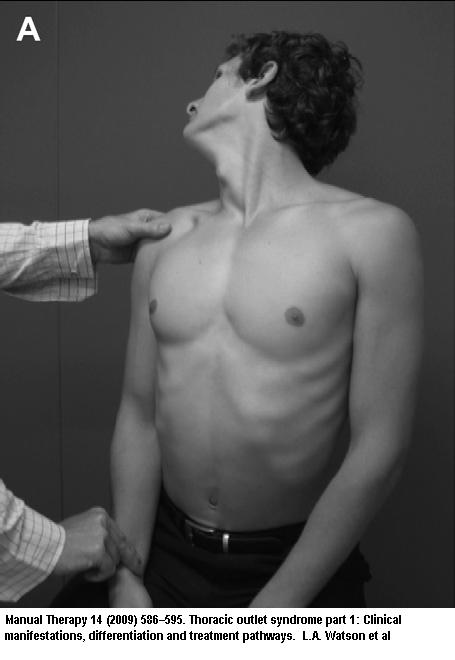
Adson test:
- Arms in lap
- Neck rotated and extended to tested side.
- Deep breath held for 30 sec while radial pulse monitored
I have seen patients with symptoms for years dismissed because no one sought these out, (and because physios do not seem to be able to take a pulse?)
5) Relief by injecting anterior scalene
Technique:
In:
Jordan SE, Machleder HI. Diagnosis of thoracic outlet
syndrome using electrophysiologically guided anterior
scalene blocks. Ann Vasc Surg 1998;12(3):260–4.
Injection of the muslce was as follows:
- “ASM was identified deep to the sternocleidomastoid muscle and could be activated withlateral neck bending against resistance and with deep inspiration.”
- “needle advanced through the sternocleidomastoid muscle above the subclavian pulse and directed in a sagittal plane, lateral to the carotid pulse.”
- “patient would be asked if pain was produced and whether insertion at this depth reproduced pains that were similar in quality and location to the usual pains”
- “Needle depth was typically within a range of 2 to 4 cm depending on body habitus”
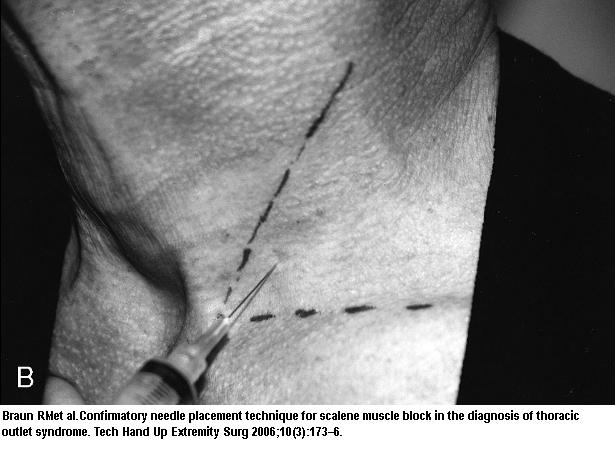
Another Approach by:
Braun RM, Sahadevan DC, Feinstein J.
Confirmatory needle placement technique for scalene muscle block in the diagnosis of thoracic outlet syndrome.
Tech Hand Up Extremity Surg 2006;10(3):173–6.
- Mark clavicle and posterior border sternomastoid
- Anterior Scalene descends medially to under SM at a 30 degree angle to such.
- “site for the injection is approximately 2 fingerbreadths above the clavicle at the lateral edge of the sternomastoid muscle along the line of scalene descent onto the first rib.”
- The injection approaches from the lateral border of the sternomastoid muscle, at a slightly cephalad, slightly medial angle.
- It would have been nice if two fingers could have been put on either side of the anterior scalene and injection between the two as per video near end.
- With syringe detached, the needle placement confirmed by watching.
“synchronous needle motion” associated with patient deep respirations.
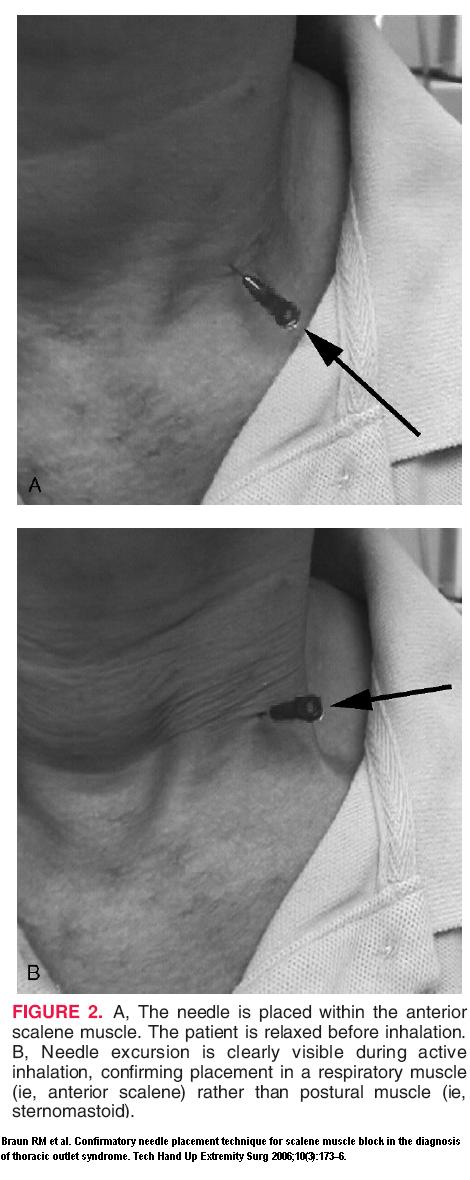
- Injection local should give pain relief within 10 minutes without sensory block (which would indicate brachial plexus block). The above used 4-5 mls of 1% lidocaine. If you want something short acting, you could use Nasacaine which lasts 15-30 minutes.
Need for Middle Scalene Botox Injection and More
-
- In above study they only injected Botox in the anterior scalene which I think was a mistake.This article felt the medial scalene was also important:
-
- Scalene Muscle Abnormalities in Traumatic Thoracic Outlet Syndrome
-
- Richard J. Sanders et al
-
- THE AMERICAN JOURNAL OF SURGERY VOLUME 159 FEBRUARY 1990. 231-236
-
- They state:”The anterior scalene muscle was identified as the site of abnormality in the scalenus anticus syndrome by Adson and Coffey [11] in 1927. Twenty years later, the middle scalene was recognized as another source of abnormality [12]. In this study of 45 scalenectomies, fibrosis
-
- (defined as more than 20% connective tissue) was present in 97% of anterior and 77% of middle scalene muscles. Type II fiber atrophy and type I fiber predominance was observed in 72% of the anterior and 51% of the middle scalene muscles.
Thus, middle scalene muscle involvement
was almost as frequent as anterior scalene involvement.
-
- The clinical significance of these observations of middle scalene pathology is that this muscle probably should be excised along with the anterior scalene muscle when scalenectomy is performed. This is particularly true when the patient has symptoms in the C8 distribution, as
the
middle scalene muscle has often been observed to press against this nerve, whereas the anterior scalene seldom does
-
- . In performing transaxillary first-rib resection, the middle scalene, as well as the anterior scalene muscle, is always transected. Failure to divide the middle scalene muscle at the time of scalenotomy might explain why, in some series, transaxillary rib resection has shown better results than anterior scalenotomy alone. “
In:
Pain Physician 2007; 10:541-546.
Combining Ultrasonography and Electromyography for Botulinum Chemodenervation Treatment of Thoracic Outlet Syndrome: Comparison with Fluoroscopy and Electromyography Guidance
Sheldon E. Jordan, MD1, Sam S. Ahn, MD2, and Hugh A. Gelabert free article here
They injected Scalene anterior and middle, later they added the subclavius and pectoralis minor muscles.
“For the anterior scalene muscle 12 units of Botox were injected, for the middle scalene muscle 12 to 15 units were injected. Twenty-five units were injected into the subclavius and 35 units were injected into the pectoralis minor. All patients received an additional 75 to 100 units into painful and dystonic neck and shoulder muscles including the trapezius and levator scapula.”
A good outcome was over a 50 percent improvement in pain plus a reduction in use of painkillers, combined with self reported improvements in arm functioning. 81 – 91% acheived these results.
Subclavius is a little muscle just below clavicle. I had never heard of it being injected for TOS before.
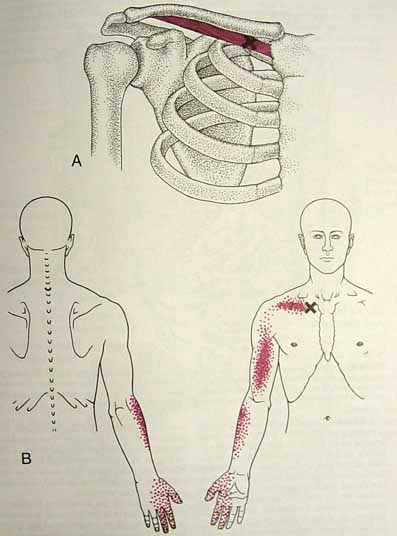
(pic originally from Travell & Simon’s book)
The pectoralis minor has been the topic of injection by Dr. David Simons years ago:
Response to Treatment for Pectoralis Minor Myofascial Pain Syndrome After Whiplash
Chang-Zern Hong ; David G. Simons
Journal Of Musculoskeletal Pain, Volume 1, Issue 1 September 1992 , 89 – 132 abstract here
There study was pre-botox – about 1/3 would respond to grueling physio, 1/3 that didn’t respond, responded to regular injections of freezing, and 1/3 didn’t respond. The unresponders all had bulging discs in the neck on imaging.
See how pect minor can entrap
(also initially from Travell & Simon’s Book)
———————-
Injection Technique
Botox injection of Scalene is video explained here:
http://present.toxtalk.com/scalenex/launch.htm
Getting back to the original article,
Present study injected 20 units.
Results
They stated they got:
“Patients experienced substantial pain relief in months 1 and 2 following a single Botox injection into the ASM under CT guidance. Significant pain reduction was noted for 3 months after Botox injection with respect to both sensory and VAS scores, and the total and PPI scores approximated statistical significance. After 3 months, patients experienced a 29% decrease in the sensory component of their pain as well as an approximate 15% reduction in their VAS score. A single, CT-guided Botox injection into the ASM may offer an effective, minimally invasive treatment for NTOS.”
This is not as good as the Pain Physician article, but a lot less hard to do.
Comment – I hope these cases had physio to work on these muscles after injection. I also hope this article gives a clearer idea how to deal with this problem.
Addendum – I inject the anterior scalene using a 25 guage butterfly needle. It gives me control and doesn’t go too deep. I still watch for it going up and down with respiration. I use 2 cc lidocaine 1% and 1 cc kenalog 40 mg, You can readily see if there is any blood backflow.. I know I am not getting the deep part of the muscle but if I massage enough it spreads and relaxes and I can use stetches(One hand on forehead and other pushing down just right below clavicle helps). This way I don’t have to worry about neck arteries or phrenic nerves… It gives good relief for a while and is hence good diagnostically…
I would appreciate any comments on how it could be done better…
Pingback: Corn Syrup for Baby Constipation | Baby Constipation Remedies
very good article – congratulations! Do you have any opinion or exprerience using ultra-sound guidance for the Botulinum injections into the scalene muscles. Another question: a few complications have been reported about these injections into the scalenes, like dysphagia and others – do you think they are significant enough to be concerned?
Joe
Just did a couple of interscalene TPI under ultrasound, using in plane approach. First time used 0.3 ml 0.5% marcaine in the anterior and same dose in posterior. Got great relief, but sadly also got a great partial plexus block. Next time, 0.1 ml of 2% lidocaine into each one. 100% relief, no BP block. This is in a patient who had negative diagnostic blocks of cervical nerves proximal to the scalenes. Next step is botox . . . will keep y’all apprised. Am also ordering PT.
Hello,
I am a patient looking for an experienced professional to treat my pec minor and ant/mid scalene thoracic outlet syndrome with botulinum toxin. Any recommendations for Southern California or Boston? Also, I am willing to travel for quality care! Much thanks.
Hello KJC,
Dr. Morris Jagodowicz in L.A. is a wonderful pain specialist who has treated my
T.O.S. with anterior scalene blocks with botox for years. I always got great, fairly long term relief from the injections. Unfortunately, I moved to Oregon and cannot find a doctor up here who knows anything about these injections.
I am in terrible pain again and can’t afford the trip to S. CA. I miss Dr. J tremendously.
Hi KJC
Dr. Loren Fishman in NYC does Botox into scalene muscles for TOS. I highly recommend him. He is a wonderful doctor and a true expert. extremely kind and the best side manner I have ever encountered in a doctor! He uses EMG for guidance. Good luck!
Thanks DR
Because of you and this blind technique, I have 3 patients back to work in just 3 weeks.
Any idea on injecting blindly the minor pectoralis? Easier to inject the tendon, but would like to get pass the myotendinous jct and get some sort of confirmation that I am not in pec major or in the lung…
Thanks again
I have neurogenic TOS with paresthesias in the hand and face+diziness. Every time i turn my head to the opposite side i Have these symptoms. Do you know any specialist in Europe who knows how to do scalene block and botox injections?
Do you know anyone in Atlanta? Ive come to know that this problem has been mine for at least 40 years. Stretch therapy helped somewhat and exposed the issue. More intervention is needed. Thanks
Pingback: Scalene Botox Injection | New Botox Effects
Pingback: Botox In Injection Muscle Scalene | Common Botox Effects
I am interested in locating providers in the North Texas area for my clients who I serve in the home environment as I am a Physical Therapist. So much of the internet sites for chronic pain physician groups are not exposing their expertise to the general public who view their website. They only talk about steroid shots and TENS units or in some instances CES ( cranial electrical stimulation). I would appreciate some guidance about what credentials to look for when looking for a qualified provider who can treat areas like the scalene muscles; the first rib area; the quadratus lumborum; and pectoralis minor. I want someone who is very through and is using state of the art techniques, because MORE than HALF of my clients do not receive sustainable relief with a traditional steroid shot or facet block injection.
————
Don:
Sounds like you are looking for someone to do myofascial pain work. For that, I would suggest they would be a member of the
International Myopain Society
http://myopain.org/
If you are looking into more Orthopaedic medicine then:
AAOM – American Association of Orthopaedic Medicine
http://www.aaomed.org/
If you are looking for prolotherapy, then either the above one or
AOAPRM – American Osteopathic Association of Prolotherapy Regenerative Medicine
http://www.prolotherapycollege.org/
Some osteopaths may be good too but some just do traditional medicine now.
AOA – American Osteopathic Association
http://www.osteopathic.org/Pages/default.aspx
Perhaps any of these organizations might suggest people in Texas if they are willing.
As for someone good at thoracic outlet syndrome, I don’t know anybody so could use some input here…
I have not had much luck in getting people to right person – they say they saw the orthopaedic medicine doctor and were told they could do nothing (and then charged them)- So you might want to quiz the nurse to see where a doctor stands.
Good luck with that.
admin