
I recently had the following letter:
“I am doing research on use of botulinum toxin type-a in trigeminal neuralgia.so, I will be highly obliged if you will send me some details with references about dosage and techniques used in injecting different facial muscles.”
Interestingly, the use of botulinum in neuropathic pain appears to be often intradermal(injected into skin so bleb blanches skin)…
- Piovesan, E J. MD; Teive, H G. MD; Kowacs, P A. MD; Coletta, M V. Della MD; Werneck, L C. MD, PhD; Silberstein, S D. MD, FACP
An open study of botulinum-A toxin treatment of trigeminal neuralgia. Neurology. 65(8):1306-1308, October 25, 2005. abstract –
They used about 7 units BoNT/A per trigeminal division – almost a homeopathic dose!! intradermal at ill-described spaced areas
Yet they seem to get results:
- In a trigeminal neuralgia case study,
Clin Neuropharmacol. 2005 Jul-Aug;28(4):161-2.
Botulinum toxin and intractable trigeminal neuralgia.
Türk U, Ilhan S, Alp R, Sur H. abstract here
They used in their case, “100 U botulinum toxin was injected into the region of the zygomatic arch.”
good results
In a Trigeminal neuralgia study:
Arq Neuropsiquiatr. 2008 Sep;66(3A):500-3.
Beneficial effects of botulinum toxin type A in trigeminal neuralgia.
Zúñiga C, Díaz S, Piedimonte F, Micheli F. abstract here
They used:
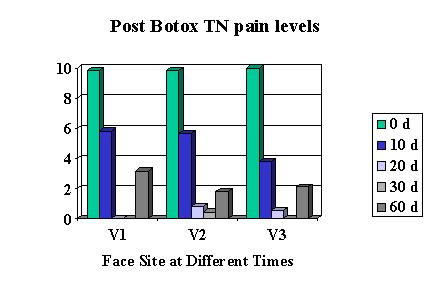
“botulinum toxin type A injections in 12 patients with otherwise unresponsive idiopathic trigeminal neuralgia. Patients were infiltrated with 20-50 units of botulinum toxin in trigger zones. Those who presented with mandibular involvement were also infiltrated in the masseter muscle.”
They state:
“Ten of our patients reported a significant benefit from botulinum toxin injections, with reduction or even disappearance of pain, and remained pain free for as long as 60 days. ” Their injections were subcutaneous
Another TN study:
- Cephalalgia. 2006 Mar;26(3):336-40.Botulinum toxin A for the treatment of greater occipital neuralgia and trigeminal neuralgia: a case report with pathophysiological considerations.Volcy M, Tepper SJ, Rapoport AM, Sheftell FD, Bigal ME.
“because of persistent left V2 TN pain….The patient was given an additional 7.5 units of BTX-A into the left masseter and zygomatic muscles, which gave him excellent pain control (more than 90% relief) over the next 2 months with consequent analgesic overuse cessation. A new series of BTX-A injections were given to the patient at the end of the fourth month of follow-up, 6 units into the left masseter and zygomatic muscles, and 12 units over the right ON area, with complete relief of pain both from GON and left V2 TN in the last three months.”
These above articles have been attacked (letters – no abstracts)
Eur J Neurol. 2009 May;16(5):e104.
Botulinum toxin for trigeminal neuralgia. Nurmikko T, Cruccu G.
An open study of botulinum-A toxin treatment of trigeminal neuralgia
NEUROLOGY 66 May (1 of 2) 2006 p1458-9; J.M. Zakrzewska, et al
- not controlled though I doubt any placebo effect could possible block tics
- not enough detail
- Wide variety of cases – some already partially treated though failures of other techniques
- variety of techniques – some intradermal, some intramuscular.
Comment – None of these criticisms in my mind nullify that they help yet have resulted in botulinum being kept off the “todo” list of TN Official recommendations. My somewhat bemused answer to this criticism is “Have they even tried it?” – because then they would at list know it makes a difference.
Other Neuropathic uses include:
- In a case of post herpetic neuralgia,
Liu HT, Tsai SK, Kao MC, Hu JS. Botulinum toxin A relieved neuropathic pain in a case of post-herpetic neuralgia. Pain Med. 2006;7:89-91. abstract here
Their study was unique – they gave their injections subcutaneously (bit deeper) and injected the material in a fan like manner.
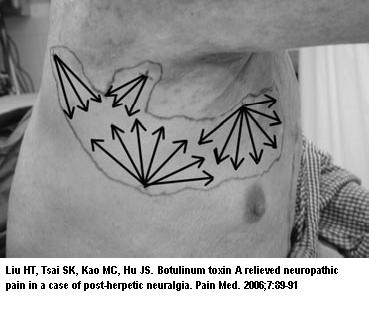
“100 units of BTX A were injected subcutaneously in a fanning fashion in divided doses (at four sites, 20 routes in total, 5 units/route) into the area of allodynia with a 23-gauge needle (0.65 × 70 mm, Nipro)”
They got 52 days relief in an intractible case.
Comment – one of the most touching cases I had was an elderly frail lady, who I saw, with fresh post herpetic neuralgia Right T8 on chest. She was in considerable pain and could not tolerate any conventional medication. Dr. Mike Lang, a very caring anesthetist, was willing to come out to Emergency one Saturday morning and give her a local anesthetic – steroid epidural injection. I held her up while she sobbed away. Following that, I gave her 100 units of Botox in multiple blebs over the hyperesthetic zones. I never heard from her again (only saw her while my partner was away). I found out from word of mouth later that she got much better and lived 6 months until her chronic leukemia flared and took her away. What I didn’t realize was how touched her son was that we went out of our away to do that – something I didn’t give a second thought to at the time…
- A Diabetic foot neuropathy study,
-
-
- have used 100 units in 1 cc saline injected over the area marked out as the zone of referral.
- Obviously if there is a trigger zone this should be given special attention.
- The muscles do play a role in the sensization to the area and hence any sensitive msucles need attention as well – like above where they say if the mandibular division is involved they inject the masseter. and there was mention of injecting zygomaticus as well – at least 6 units each.
- I have put the intradermal blebs twice as close as the foot example imaged above though I do not know if this is necessary.
- It takes a week for the results so I know it is not placebo, and it can wear off very alarmingly in 10-12 weeks.. Please, please, please – make arrangements for reinjection at least at 8-10 weeks otherwise the resurgence can be poorly tolerated.
- There is a risk of asymmetric wrinkles and drooping eyelid if given too close to the eye. I must have hit a nerve in one case and it flared things after – so make sure you stay very close to the skin…
- It seem that the use of much less, as evidenced by one article, would be be more cost effective. The cases I had were desperate and you only get one chance ie – doesn’t work first time? – no one is ever touching my trigger zones with a needle ever again….
- Important tip – even with no air in the syringe, when you remove the needle from the skin, there is lost fluid in the form of a drop on the needle that develops between needle placements. I have been told to pull back on the syringe before removing it but find that doesn’t work that well. The best I have found is to pull the needle out and re-insert amost immediately in a new site before a bleb forms …. good luck with that.
- failed right posterior fossa exploration
- 100 units of botulinum toxin type A (BOTOX) diluted in 2.5 mL saline
- 60 units into nasal trigger zone and 40 units into mental nerve severe zone
- 5 months relief to nasal and in part mental.
- repeat block and tegretol took it from there for 1 year
- had stereotactic gamma knife radiosurgery then
- Dental case with pain and numbness chin
- 10 units Botox used as can see deep subcut
- significant decrease in pain – I suspect would have been better if more used…
-
Neurology. 2009 Apr 28;72(17):1473-8. Epub 2009 Feb 25.
Botulinum toxin for diabetic neuropathic pain: a randomized double-blind crossover trial.
Yuan RY, Sheu JJ, Yu JM, Chen WT, Tseng IJ, Chang HH, Hu CJ. abstract here
They used:”Fifty units of BoNT/A in 1.2 mL 0.9% saline were then administered intradermally into each foot, with each injection comprising approximately 4 U BoNT/A (BOTOX), 0.10 mL, using a 5/16-inch, 30-g needle.”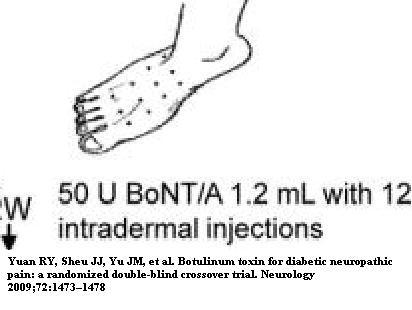 Results included decreases in pain Visual analogue scale from 0-10 decreases:
Results included decreases in pain Visual analogue scale from 0-10 decreases: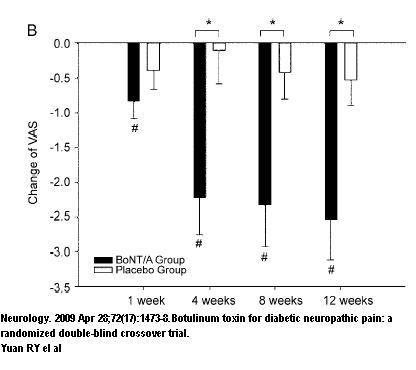
Comment – I have used Botox in trigeminal neuralgia. I prefer to use the semi-neurolytic spinal 5% lidocaine or pontocaine as discussed under trigeminal neuralgia here
Addendum:
Two article have come out re Trgeminal issues that hi-light the imporance of Botulinum ot the trigger zones:
Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Mar;109(3):e47-50.
Injection of botulinum toxin type A (BOTOX) into trigger zone of trigeminal neuralgia as a means to control pain.
Ngeow WC, Nair R. abstract
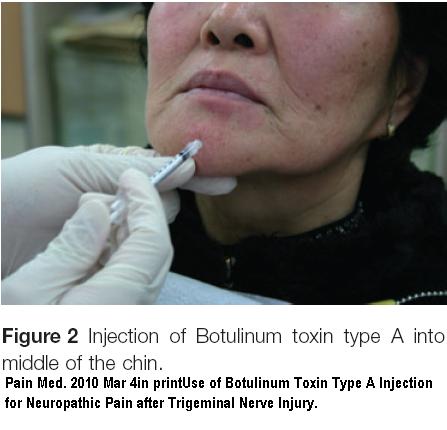
Pain Med. 2010 Mar 4. [Epub ahead of print]
Use of Botulinum Toxin Type A Injection for Neuropathic Pain after Trigeminal Nerve Injury.Yoon SH, Merrill RL, Choi JH, Kim ST. abstract here
Addendum – Botox for trigeminal neuralgia got a boost from article finding injection into trigger zones can give lasting relief – see:
Confirmed – Botox works for Trigeminal Neuralgia – Given Into Trigger Zone
Maybe will have to concentrate more on trigger zone let say in conditions like occipital and post herpetic neuralgia…
- It would help the medical community if others would be willing to share on this topic as the literature is sparse…
Hi – came across this blog post while searching for info on botox for post herpetic neuralgia. Your story about that frail old woman could be my mother’s story. (Over two years now with pain and unable to tolerate conventional meds, having pain still despite an implanted spinal stimulator, though it has helped a bit).
Do you know of anyone in the Philadelphia-NYC area who has experience/success with botox in such situations?
You cam email me directly if you’d prefer at the email above.
my mom suffered from severe trigeminal neuralgia, she found relief from botox injection. Here is her story
http://www.youtube.com/watch?v=90FZUTIUd1Y
i need to find someone to do this for me.. I have post herpetic neuralgia for over 2 years. i live in minnesota. St. paul/minneapolis area. please find me a dr.!!! depserpate for relief.
Sandy, My mother is trying Botox now for a 14 month case of post herpetic neuralgia in her foot and leg. She is going to a dermatologist who does botox. He has little experience with treating for pain but is willing to try. Will let you know how it works. I hope you get some relief soon.