
There was recent mention on using IV Magnsium in acute migraines in a previous blog note. I had used it in combination 1-2 gms Magnesium sulphate with lidocaine 100 – 200mg IV for migraines but was not impressed that it worked for that long. If given too fast, it could also cause some burning in the blood vessels in the arm used which did seem distressing. I was using a small volume that I could give slow push rather than putting it in 250 mls saline so concentration could be the cause. However, this is has encouraged me to review the use of IV magnesium: – in neuropathic, migraine, and regionally. ,
Warning: – both lidocaine and magnesium can promote AV Block and should not be used in people with such (even if first degree = prolonged PR interval)
1) In Neuropathic pain:
a) Br J Anaesth. 2002 Nov;89(5):711-4. Comment in: Br J Anaesth. 2003 Aug;91(2):302; author reply 302. Efficacy of intravenous magnesium in neuropathic pain. Brill S, Sedgwick PM, Hamann W, Di Vadi PP.
full article
- Chronic Post Herpetic Neuralgia cases
“assigned randomly to receive either an i.v. infusion of 0.9% saline 100ml
or magnesium sulphate 30 mg kg±1 (magnesium 0.06 mmol kg±1) over 30 min (the required amount was added as a 50% magnesium sulphate solution to 100 ml of saline).”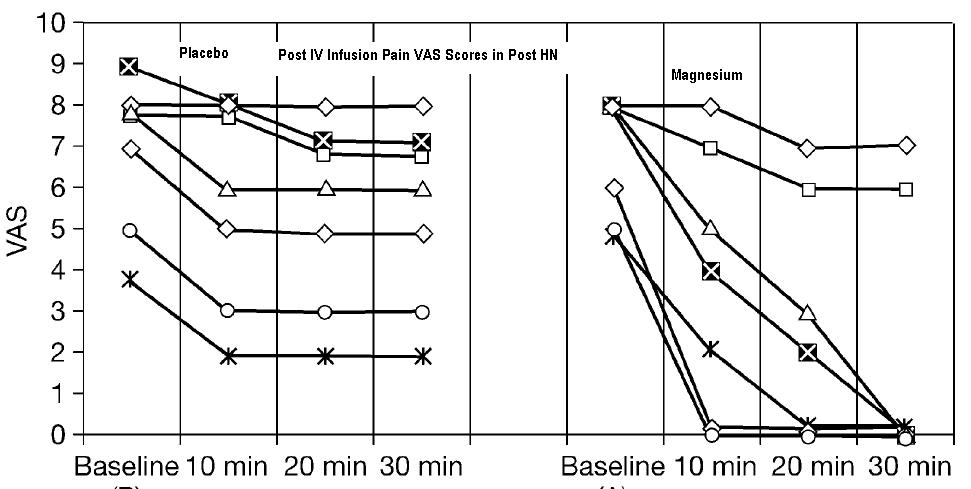
- In this one shot study helped 4/6 but the pain came back by that evening.
—–
b) Masui. 1998 Sep;47(9):1109-13.
Relief of neuropathic pain with intravenous magnesium Tanaka M, Shimizu S, Nishimura W, Mine O, Akatsuka M, Inamori K, Mori H. abstract
“post herpetic neuralgia or causalgia etc.”
“After the nerve block, magnesium sulphate (0.5 mol.l-1) 5 ml was administered intravenously by bolus infusion taking 5 min, followed by continuous infusion of the same dose for one hour”
How many grams Magnesium Sulfate in 1 moles? The answer is 120.3676.
so using 0.5 m/liter = 60 gm/liter = 6/100 = 6%. So 10 mls total would be .6 gm – not very much
“All patients were treated with this therapy once a week. In 4 patients, VAS score decreased 3 points or more when this therapy had been administered 3 to 11 times. In 2 patients, VAS score did not change, and the analgesic effect of magnesium was not certain in other 2 patients.”
Wow – makes me realize how the one-shot wonder mentality has affected thinking on magnesium – no one else bothered to repeat it and see what benefits could result.
However I am not sure what they meant by nerve block; and if it is a regional one, then this could explain the results. This was reviewed in an editorial and no mention was made of the nerve block part…
Their conclusion makes no mention of any nerve block so maybe none was done regionally: “We conclude that this therapy with magnesium once a week is safe and effective for relieving neuropathic pain.”
Worked here but suspect more in the post-herpetic neuralgia ones which are easy to control.
———
c) J Pain Symptom Manage. 2000 Jan;19(1):35-9. The safety and efficacy of a single dose (500 mg or 1 g) of intravenous magnesium sulfate in neuropathic pain poorly responsive to strong opioid analgesics in patients with cancer. Crosby V, Wilcock A, Corcoran R. abstract
- 12 patients with neuropathic pain due to malignant infiltration of the brachial or lumbosacral plexus
- both 500 mg and 1000 mg effective in 4/12 temporality complete, 6/12 partial. Unfortunately pain was back in 4 hours. Besides a feeling of warmth – no side effects
“One ml or 2 ml of 50% w/v magnesium sulfate… given intravenously over 5 or 10 minutes (500 mg or 1 g, respectively).”
- Not sure I could get away with giving Magnesium IV that concentrated without getting arm burning pain – but these subjects were on a lot of painkillers…
—
Pain. 1996 Feb;64(2):283-91. NMDA receptor blockade in chronic neuropathic pain: a comparison of ketamine and magnesium chloride. Felsby S, Nielsen J, Arendt-Nielsen L, Jensen TS.
They picked the hardest ones:
Neurectomy/neuroma -1
saphenous neuropathy – 1
sensory polyneuropathy – 1
post-thoracotomy – 3
ampuation -3
post radiation plexopathy -1
10 min bolus infusion… magnesium: 0.16 mmol/kg) followed by a continuous infusion …magnesium: 0.16 mmol/kg/h).
OK – here are my calculations:
so 70 kg would 11.2 mmol or .0112 m
1 mole Magnesium Sulfate = 120.3676 gms
so .0112m = 1.35 gms
so 1.35 gm initially and 1.35 gm continuous
conc – 100 mmol/liter = .1m/liter = 12.04 gm/liter = 1.2 gm/100ml = 1.2%
so 1.35 gm would be 112.5 mls of 1.2% = 100mmol/liter
112.5 mls bolus over 10 minutes and then 112.5 mls over rest of the hour.
They used an infusion pump.
Total dose would have been 2.4 gm for 70 kg.
point out serum Magnesium should not go over 3 mmol/liter to avoid toxicity
Magnesium did not reduce the amputation group at all.
Helped 1/3 post thoractomy; On the whole, “Mg +2 on the other hand, failed to show a significant reduction in VAS score (29%, P = 0.084) and on the area of allodynia”
Failed on the tough ones…
Comment – It appears that if looking for any longterm effect, are committed to giving the magnesium sulphate maybe 500-1000 mg bolus over 5 – 10 minutes in 20 mls saline followed by maybe 1 gm over 50 minutes. This would have to be given 3-11 times – particularly in people in which there was a definite temporary response. Suspect one would get even better results if small doses of Ketamine were used but that is another story.
2) In headaches:
Headache. 2001 Feb;41(2):171-7. Efficacy of intravenous magnesium sulfate in the treatment of acute migraine attacks. Demirkaya S, Vural O, Dora B, Topçuoğlu MA. abstract
“Fifteen patients received 1 g intravenous magnesium sulfate given over 15 minutes. The next 15 patients received 10 mL of 0.9% saline intravenously. Those in the placebo group with persisting complaints of pain or nausea and vomiting after 30 minutes also received 1 g magnesium sulfate intravenously over 15 minutes.”
“Our results show that 1 g intravenous magnesium sulfate is an efficient, safe, and well-tolerated drug in the treatment of migraine attacks.”
—-
CJEM. 2004 Sep;6(5):327-32. Intravenous magnesium for acute benign headache in the emergency department: a randomized double-blind placebo-controlled trial. Frank LR, Olson CM, Shuler KB, Gharib SF
“We found no statistically significant difference between groups for any secondary outcomes; however, the patients who received magnesium had significantly (p = 0.03) more side effects than did those in the placebo group.”
I think this was one of the articles that dissuaded me from using it. However, in reality combos are being used, so this does not tell us the whole story. One pro, one con – anyone have the best of three?
3) Regional Blocks
Anesth Analg. 2005 Apr;100(4):1189-92. Intravenous regional anesthesia using lidocaine and magnesium. Turan A, Memiş D, Karamanlioğlu B, Güler T, Pamukçu Z full article
10 mL of 15% magnesium sulfate (12.4 mmol) plus 3 mg/kg lidocaine 0.5% diluted with saline to a total of 40 mL in group
This would come to 1.5 gm Magnesium sulfate and 210 mg lidocaine for a 70 kg (in 40 mls total after saline dilution)
“Sensory and motor block onset times were shorter and recovery times were prolonged in group M (P < 0.05). VAS scores of tourniquet pain were lower in group M [magnesium added to lidocaine] at 15, 20, 30, 40, and 50 min (P < 0.001). Anesthesia quality, as determined by the anesthesiologist and surgeon, was better in group M (P < 0.05). Time to the first postoperative analgesic request in group C was 95 +/- 29 min and in group M was 155 +/- 38 min (P < 0.05). Postoperative VAS scores were higher for the first postoperative 6 h in group C (P < 0.05). Diclofenac consumption was significantly less in group M (50 +/- 35 mg) when compared with group C (130 + 55 mg) (P < 0.05). We conclude that magnesium as an adjunct to lidocaine improves the quality of anesthesia and analgesia in IVRA.”
so it obviously has some regional anesthetic effects
Pain 99 (2002) 235–241
Magnesium bier’s block for treatment of chronic limb pain: a randomised, double-blind, cross-over study
Martin R. Trame`ra,*, Chris J. Glynn
- Chronic limb pain >1 month
- Regional block technique – start IV, lift arm and tensor to drain it, apply double BP cuff like device, (use outer cuff until gets sore then inflate inner one and deflate outer)
- “They received once 20% magnesium sulphate (500 mg) 1 lignocaine 1% (75 mg), and once physiological saline 1 lignocaine 1% (75 mg). The volume of both treatments was 10 ml. “
Types:
post fracture – 3
DM neuropathy – 1
lymphoma with digit ulcerations – 2
trauma and surgery – 12
peripheral neruopathy – 1
Raynauds – 2
leg ulcer – 1
elbow overuse pains – 2
wrist and elbow NYD pains – 2
Results:
very good = 5/24
good – 8/24
(versus 3/24 good and 3/24 very good for plain lidocaine control group)
mean duration – 23 days (7.7-40)
52% found the Magnesium – lidocaine painful
There was a warm flushing all over when tournique released.
Comment – guanethidine regional block were apparently effective too. Looks like has potential but might need to give some painkiller ahead of time…
Addendum – repeated IV magnesium found helpful in Complex regional pain. Discussed here:
New Hope For Complex Regional Pain Syndrome I – 5 days Magnesium Infusions
Magnesium in depression discussed here:
Would Magnesium Help Depression ?
Anyone had more experience with IV magnesium?