
Are these legitimate arguments?
1) One shot should fix it and if it doesn’t then that’s it (I call this the “one shot wonder” attitude). I think the only person who could be sure to fix things at one go would have to be God and I know I’m not him/her…
2) Steroid injection rots the cartilage from joints and accelerates osteoarthritis. If steroid injections are used to treat symptomatic mensicial tears, I would not think repeated injections would not be the best idea as accelerated deterioration would be happening anyway.
But evidence do we have?
1) Repeated shots sustain improvement without joint deterioration over two years:
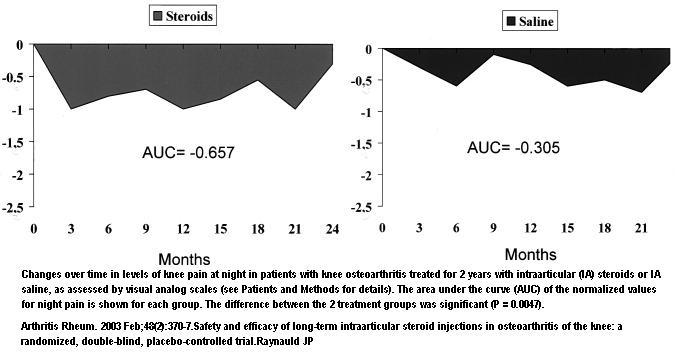
Arthritis Rheum. 2003 Feb;48(2):370-7.
Safety and efficacy of long-term intraarticular steroid injections in osteoarthritis of the knee: a randomized, double-blind, placebo-controlled trial.
Raynauld JP, Buckland-Wright C, Ward R, Choquette D, Haraoui B, Martel-Pelletier J, Uthman I, Khy V, Tremblay JL, Bertrand C, Pelletier JP.abstract
- injections of triamcinolone acetonide 40 mg (34 patients) or saline (34 patients) into the study knee every 3 months for up to 2 years.
- no xray changes
- “knee pain and stiffness were significantly improved throughout the 2-year study by repeated injections of triamcinolone acetonide, but not saline (P < 0.05)”
- no deleterious effects
- As one can see below, the shots seem to last a few months and a repeat shot sustains it:Plots of improvement:
Cochrane confirms short term benefits but states” The short-term benefit of IA corticosteroids in treatment of knee OA is well established, and few side effects have been reported. Longer term benefits have not been confirmed based on the RevMan analysis. – I suspect what they are saying is they don’t know much beyond fact repeated shots are necessary to maintain benefits.
Cochrane Database Syst Rev. 2006 Apr 19;(2):CD005328. Update of: Cochrane Database Syst Rev. 2005;(2):CD005328. Intraarticular corticosteroid for treatment of osteoarthritis of the knee. Bellamy N, Campbell J, Robinson V, Gee T, Bourne R, Wells G.
The repeated shot article did seem to set a new standard for care: A recent Cleveland clinic article stated: ” Steroid injections may be given up to three or four times per year. ”
free article
2) Hip shots are helpful:
Arthritis Rheum. 2007 Jul;56(7):2278-87.
Steroid injection for osteoarthritis of the hip: a randomized, double-blind, placebo-controlled trial. Lambert RG, Hutchings EJ, Grace MG, Jhangri GS, Conner-Spady B, Maksymowych WP.
Following hip injection they stated:
“Following injection ofthe hip, the patient was instructed to rest, preferably in the form of bed rest, for 3 days and to maintain at least minimal activity. After this 3-day period, activity was restricted for 1 week, during which the patient was asked to refrain from active exercise and, if possible, to refrain from work.”
Their conclusion was:
” This placebo-controlled trial confirms that corticosteroid injection can be an effective treatment of pain in hip OA, with benefits lasting up to 3 months in many cases. Future studies should address questions related to the benefits of repeated steroid injection and the effects of this treatment on disease modification. ”
I have a lady with a bad hip that one injection gave sustained relief – of course it helped that she was light-weight…
Comment – It looks like the new standard is to repeat shots in the knee four times a year but the hip is anyone’s guess. The safe dose was 40 mg Triamcinolone – not 80 mg like I have seen rheumatology use..
Any comments here?
I have OA in my knees, I have been doing Deep Water Workouts at the local pool; 95% of my pain is gone; prior to this, I was limping and had a hard time going up the stairs; Deep Water Workouts strengthen the muscles in the upper and lower leg, thus strengthening the knee joint.
It’s fantastic.
P.S.
I would NEVER allow steroid injections as a bandaid for symptomatic relief;
Being proactive is the answer – join up for Deep Water Workouts
There is no strain or stress to the joints, and the OA is thereby naturally treated – pain goes away for the most part.
Check out the web for any information related to Osteo Arthritis, as well, look up ‘Deep Water Workout’.
There is a new procedure called Radio Frequency Ablasoin Denervation. It burns the selected nerve with high frequency sound. It is a needle based minimally invasive procedure. It lasts about a year until the nerve grows back. I have just had fecet steroid injections as a definitive diagnosis. On to the next step. There is also a Lazer Ablasion that is permenant. As the Boombers all get old and achy we can’t fix old age. Trying to fix it all will bust the budget. Just stop the pain, so we can feel young until we die.
Thank you. This is just the information I was looking for. I was wondering if the steroids would degenerate the cartilage and how long I should get the steroid shots before I go for an Ablasion.
There is a new procedure called Radio Frequency Ablasoin Denervation. It burns the selected nerve with high frequency sound. It is a needle based minimally invasive procedure. It lasts about a year until the nerve grows back. I have just had fecet steroid injections as a definitive diagnosis.
There is also a Lazar Ablasion that is permanent. As the Boombers all get old and achy we can’t fix old age. Trying to fix it all will bust the budget. Just stop the pain, so we can feel young until we die.
Pingback: Pain Medical Musing Blog Archive Steroid Joint Injection | Joint Pain Relief
I think your blog post was really a good kick off to a potential series of articles about this topic. So many bloggers pretend to understand what they’re preaching about when it comes to this area and most of the time, hardly anyone actually get it. You seem to grasp it however, so I think you should run with it. Thanks a lot!
I realize this is a very old strand, but wanted to put my two cents in anyway. I suffer quite badly from Ehlers-Danlos Syndrome. Many of my joints are in constant pain, but my hips have always been the biggest source of pain as well as constant dislocations. I receive steroid injections in my hips and shoulders as well as many trigger point shots in my back, at least every three months and sometimes as often as every other month. I completely understand the long term risks, but in life we are offered choices. I choose quality of life over quantity, meaning. I would rather be able to walk for a few days every few months after my shots, then extend my time later suffering in pain after my hips are completely gone and I can never walk again. My joints are degenerating no matter what, as is my over all health, there is no treatment for what I have and no way to stop it. Therefore I thankfully accept the gift of mobility that steroid shots give me while I am still able to enjoy that gift.
Perhaps my situation is unique and does not apply here, but maybe it does, or maybe it might give someone rigidly against the idea of some treatment that comes with the risk of side effects a different way of looking at the positive as well as the negative. Something to think about anyway.
Pingback: Medial Knee OsteoArthritis (OA)- What Else Can You Do? – Unload it and more | Pain Medical Musing